Stewart, Vigil, Olszewski, and Thornock: Gesture use in children with autism spectrum disorder: a scoping review
Abstract
Purpose
This study reviewed the literature examining type and frequency of gesture use in children diagnosed with autism spectrum disorder (ASD) in comparison to other populations. The findings can inform future studies and programs targeting the use of gestures as an early indicator of ASD.
Methods
A six step search procedure was utilized to identify all articles exploring gesture use in children with ASD in comparison to other populations. Articles meeting inclusion criteria were double coded by the investigators with 97% agreement. Results examining type and frequency of gesture were synthesized and three common themes were identified: comparison group(s), age of participants with ASD, and gesture terminology.
Results
A total of 32 studies met inclusion criteria for this study. Of these studies, nine exclusively measured type of gesture, 17 exclusively measured frequency, and 6 measured both type and frequency. Results indicate that children with ASD used different types and frequency of gesture in comparison to other populations. The most studied age range was 4–5 years and most studies used typically developing children as the comparison group. Gesture terminology and definition were extremely variable.
Conclusions
Children with ASD are using different types and frequencies of gesture when compared to other populations. More research including younger and more diverse populations is needed to translate these findings into clinical practice. Additionally, there is a need for more consistent use of gesture terminology and definition.
Keywords: Autism spectrum disorder; Gesture; Early identification; Gesture type; Gesture frequency
INTRODUCTION
Research in gesture use in children with autism spectrum disorder (ASD) shows delays and differences in the quantity and quality when compared to other populations [ 1– 3]. These delays and differences are evident prior to a child’s first birthday, placing lack of or atypical gesture use as one of the earliest behavioral markers of ASD [ 4– 6]. Although lack of and atypical use of gesture use can be identified during the first year of life, the average age of diagnosis of ASD is currently 4 years, 2.5 months [ 7]. If gestures can be accurately used to identify children with ASD prior to their first birthday, children can receive diagnoses and begin receiving early intervention at much younger ages, resulting in better outcomes for this population [ 8, 9]. Even though gestures have been consistently identified in the literature as one of the earliest indicators of ASD, to this date, a review has not been conducted comparing findings across studies. This information is of interest for research purposes and clinical practice as it can help to inform the current state of the literature, identify strengths and weaknesses of children with ASD, and summarize findings so that research can be translated into clinical practice. Taken together, this can aid in identification of ASD at a much younger age than the current average of 4 years, 2.5 months [ 7]. Consequently, the purpose of this study is to evaluate the research examining gesture use in children with ASD in comparison to other populations with a focus on type and frequency of gestures. We will address the following research questions:
Do children with ASD use different types of gesture in comparison to other populations? Do children with ASD use different frequencies of gesture in comparison to other populations?
METHODS
Search procedure
A six-step process was used to conduct a scoping review of the literature related to gestures and ASD. First, the authors identified five primary and 21 secondary search terms. The five primary search terms were autism, autism spectrum disorder, autistic disorder, Asperger’s, and PDD-NOS. The 21 secondary search terms were gestures, instrumental gesture, representational gesture, iconic gesture, deictic gesture, conventional gesture, showing, giving, pointing, commenting, protesting, acknowledging, social interaction gesture, behavior regulation gesture, joint attention, intention, nonverbal communication, preverbal communication, and gesture development. All possible two and three primary and secondary search term combinations were entered into each of five electronic databases: PubMed, Web of Science, Academic Search Premier, PsycInfo, and ERIC.
Second, the authors and trained undergraduate research assistants conducted abstract reviews to determine if articles identified in step one “met” or “potentially met” inclusion criteria. Articles investigating eye movements in isolation, social smiles in isolation, gestures trained by the investigator(s) or imitated by the participant, and studies measuring gestures via parent interview were excluded. Duplicate abstracts and abstracts that did not contain the search terms were eliminated.
Third, full-text articles of all the abstracts identified as “met” or “potentially met” were obtained for article review. Below were the inclusion criteria:
Peer reviewed studies with experimental, quasi-experimental, case study, or single-subject design. Study participants including children between the ages of 6 months to 6 years diagnosed with ASD, Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS), Asperger’s disorder, and/or autistic disorder. A comparison group was included in the sample of participants. Studies included one or more dependent variables specific to the definition of gesture used in this current scoping review, that is—intentional movements that are interpretable by other individuals and used for the purpose of communicating meaning [10]. Gestures were measured in isolation or in conjunction with vocalizations, social smile, and/or eye contact.
Fourth, the authors conducted a full-text review of the articles identified in step two to determine if they met inclusion criteria. The articles were evenly divided amongst authors and independently evaluated. Articles that met inclusion criteria were saved for coding later. Articles that did not meet inclusion criteria were eliminated. Discrepancies were resolved by group consensus.
Fifth, an undergraduate research assistant completed an ancestral search. All references to the articles identified in step four were reviewed for inclusion criteria. No additional articles were identified in this step.
Sixth, articles that met inclusion/exclusion criteria were double coded by the authors based on the coding procedure outlined below.
Coding procedure
A coding procedure was developed to analyze content of selected articles based on the recommendations of What Works Clearinghouse Procedures Standards Handbook Version 3.0 and Cooper, 2009 [ 11, 12]. The following information was extracted from each study:
Study information: author(s), year of publication, and funding source. Participant information: socioeconomic status (SES), parent education, race, gender, diagnosis, criteria for diagnosis, age, study’s participant inclusion criteria, and group assignment and characteristics. Gesture information: terminology, definition(s), gesture description, material(s), communicative partner, and larger construct(s). Study design: length of session or observation time, location of data collection, and research design. Results pertaining to gestures. Statistical analysis used in the study.
Intercoder reliability
The authors double coded all articles that met inclusion criteria. Intercoder reliability was calculated by dividing the number of item agreements by the total number of potential agreements. An interrater agreement of 85% or better was considered acceptable. If the article did not meet this agreement, the authors resolved discrepancies. There were no articles that did not meet 85% or better. The overall percentage of agreement across the coders was 97% (1,758 agreements divided by 1,821 potential agreements).
Data synthesis
Articles that met inclusion criteria were placed into two categories: 1) those that examined gesture type and 2) those that examined gesture frequency. Gesture ‘type’ was defined as the presence, absence, or specific attributes of a gesture. Gesture ‘frequency’ was defined as quantity or number of gesture(s) per given time. If an article examined both type and frequency, the article was included in both categories.
Next, a qualitative review of all articles was conducted to identify common themes useful for comparison of findings across articles. Three common themes emerged: 1) comparison group(s), 2) age of participants with ASD, and 3) gesture terminology. Results were analyzed separately according to these three themes.
For the comparison theme, there were four frequently occurring comparison groups across the studies: 1) typically developing, 2) pervasive developmental disorder and/or pervasive developmental disorder, not otherwise specified, 3) intellectual developmental disorder/intellectual disability, and 4) developmental delay/developmental language delay and/or language delay. These comparison groups were used to synthesize results of the current study to determine differences in types of gesture or frequencies of gesture. It should be noted here that an ‘other’ category was included for studies using comparison groups not represented by the aforementioned categories.
For the “age of participants with ASD” theme, studies were placed in one year increments up to the age of 6 years. A category was added for 6 years and above for studies that included older participants. If data was collected retrospectively, the participants were placed in the age of the participant at the time of data collection. The age of participants with ASD was synthesized to determine the differences in types of gesture or frequencies of gesture by age.
For the gesture terminology theme, all gesture terms used across studies were examined for similarities. We could not synthesize this information due to extreme variability in gesture terminology used across studies. A discussion will be provided.
RESULTS
Literature search
The final sample included 32 studies published between 1978 and 2014. The initial broad search identified a total of 49,798 titles. Abstracts of these articles were reviewed according to inclusion criteria. Duplicates and abstracts failing to meet the specified inclusion criteria were eliminated, resulting in 451 abstracts. Full articles of these abstracts were obtained and reviewed to evaluate whether they met inclusion criteria. Articles that did not meet inclusion criteria were eliminated, resulting in 32 articles. An ancestral search was conducted on the remaining 32 articles with no additional articles identified ( Figure 1).
Final sample characteristics
The final sample included 32 studies. All 32 studies were non-experimental, of which seven were retrospective. Of the 32 studies, nine exclusively measured type of gesture, 17 were found to exclusively measure frequency, and six studies measured both type and frequency. No funding trends were noted across all articles.
Gesture type studies
A total of 15 studies (9 that measured type of gesture only and 6 that measured type and frequency) were analyzed to answer the first research question regarding type of gesture used in children with ASD in comparison to other populations. Of the 15 articles included, 14 found that children with ASD used significantly different types of gesture when compared to other populations ( Table 1).
Comparison group(s)
Across the gesture type studies, the most utilized comparison group was typically developing (n=8) followed by developmental delay/developmental language delay/language delay (n=6), pervasive developmental disorder, not otherwise specified (PDD-NOS) (n=3), and intellectual developmental disorder/intellectual disability (n=2). Comparison groups represented in the ‘other’ category were Down syndrome, fetal alcohol spectrum disorder, William syndrome, and regulatory disorder ( Table 1).
Age
Across the gesture type studies, the study samples most frequently included children 4–5 years of age (n=10), followed by 3–4 years of age (n=7), 5–6 years of age (n=6), 6 years of age or more (n=5), 2–3 years of age (n=4), 1–2 years of age (n=3), and 0–1 years of age n=2) ( Table 1).
Gesture terminology
Across the gesture type studies, a total of 38 gesture terms were used in the 15 articles included in this scoping review. Thirty of the 38 terms were different. Further analysis of results based on gesture terminology was not possible due inconsistency across studies ( Table 1).
Gesture frequency studies
A total of 23 studies (17 that measured frequency only and 6 that measured frequency and type) were analyzed to answer the second question regarding frequency of gesture use in children with ASD in comparison to other populations. Results were mixed in terms of frequency of gesture use in comparison to other populations. Some studies found that children with ASD gestured more frequently, some found children with ASD gestured less frequently, and others found no difference. Result varied dependent upon gesture type examined, comparison group, and age of participants with ASD ( Table 2).
Comparison group(s)
Across the gesture frequency studies, the most utilized comparison group was typically developing (n=15) followed by developmental language delay/language delay/developmental delay (n=9), intellectual developmental disorder/intellectual disability (n=6), and pervasive developmental disorder/pervasive developmental disorder, not otherwise specified (PDD/PDD-NOS) (n=3). Comparison groups represented in the ‘other’ category were Down syndrome, hyperkinetic syndrome of childhood, regulatory disorder, and mixed disability ( Table 2).
Age
For age, the study samples most frequently included children 4–5 years of age (n=14), followed 3–4 years (n=12) and 5–6 years (n=10), 6 years or more (n=8), 1–2 years (n=7) and 2–3 years (n=8), and 0–1 years (n=1) ( Table 2).
Gesture terminology
Like findings from the gesture type analysis, a total of 80 gesture terms were used in the 23 studies examining frequency of gesture use in children with ASD in comparison to other populations. Sixty-two of the 80 terms were different. This made further analysis based on gesture terminology not possible ( Table 2). Given the variability of findings across studies examining frequency of gesture, an ad hoc analysis was conducted of those studies that found statistically significant differences in frequency of gesture use. Thirty-three gesture types were used significantly less in children diagnosed with ASD and six gesture types were used more frequently in children with ASD when compared to other populations ( Table 3).
DISCUSSION
The purpose of this study was to review research studies examining type and frequency of gesture use by children with ASD in comparison to other populations. Gestures have been consistently identified in the literature as one of the earliest indicators of ASD; however, to this date, a review has not been conducted comparing findings across studies [ 4– 6]. The findings are of interest for research purposes and clinical practice because they inform the current state of the literature, identify strengths and weaknesses, and summarize findings so that research can be translated into clinical practice. The findings can be used for future research and programs targeting early identification of ASD. The results for type of gesture use indicated that children with ASD used significantly different types of gesture when compared to other populations. The results for frequency of gesture use were mixed. Some studies found that children with ASD used more gestures, some studies found that children with ASD used fewer gestures, and some studies found no difference. An ad hoc analysis of studies finding significant differences in frequency of gesture use suggests that children with ASD use fewer gestures when compared to other populations. This is the first synthesis in the literature examining the type and frequency of gesture use by children with ASD in comparison to other populations. These findings can help with earlier identification of young children with ASD and support the fact that the gesture profiles of children with ASD are different than other populations.
Three common themes emerged in synthesis of the data. These themes were important not only for conceptualization of the results relating to type and frequency of gesture use in children with ASD, but they also highlighted gaps in the literature and areas in need of further investigation so research findings can begin to be translated to clinical practice. The three themes were: 1) comparison group(s), 2) age of participants with ASD, and 3) gesture terminology.
Comparison groups
For all studies include in this scoping review, the most frequent comparison group was typically developing children followed by pervasive developmental disorder, not otherwise specified; intellectual developmental disorder/intellectual disability; and developmental language delay and/or language delays. The fact that many studies have examined gesture use in children with ASD in comparison to typically developing children is informative and gives us great insight into how these two populations differ at young ages. However, ASD has multiple overlapping symptoms with other developmental disorders; therefore, if gestures are to be used as an early indicator of ASD more studies with additional comparison groups are needed. The inclusion of studies examining additional populations will allow for differential diagnosis and further our understanding of how gestures can be used as an early indicator specific to ASD.
Age of participants with ASD
For age range, the least studied population across all studies was children 0–1 year of age. This finding is interesting because in typically developing children, gestures emerge around 8–9 months and gestures are known to be one of the earliest behavioral markers of ASD [ 6]. Further, the most frequent age studied was the 4–5 years age range. This is directly in line with the average age of diagnosis of ASD reported by the CDC [ 7]. Across all studies, there was a disproportionate amount of research in the ages 2 years and older with the least amount in 2 years and younger. For example, those studies that focused on frequency, the number of studies for 2 years and older was 16 while the number of studies for 2 years and younger was 7. For type of gesture, the number of studies for 2 years and older was 11 and the number of studies for 2 years and younger was 4. This explicitly shows the need for further research in younger populations. Further studies examining the use of gesture in younger children with ASD will help us understand the initial and dominant forms of communication for this population and has the potential to lead to detection of this disorder at younger ages than is currently possible.
Gesture terminology
Lastly, we found that across all studies there was little consistency in gesture terminology being used and how this terminology was defined. In the 15 articles that examined type of gesture, a total of 38 gesture terms were used of which 30 were different. In 23 articles that measured frequency of gesture, a total of 80 gesture terms were used of which 62 were different. If researchers and practitioners are to use gestures to clinically detect ASD at the earliest possible age, it is necessary to have consistency in gesture terminology and definition. The inconsistencies identified by this scoping review directly affected our ability to make comparisons across studies and will impact the ability to translate research findings to clinical practice. There is a great need for standardized and consistent use of gesture terminology and definitions. Hopefully, these findings will begin a dialogue between researchers and practitioners to standardize gesture terms.
Limitations and directions for future research
This initial scoping review explored gesture use in children with ASD in comparison to other populations. Most studies included in this study were found to be investigating children 4–5 years of age, the most identified comparison group was typically developing children, and a need for more consistency in gesture terminology was identified. For gestures to be considered as an early indicator of ASD, there is a need for more studies exploring gesture use in younger populations. Furthermore, there is a great need for future studies including comparison groups other than typically developing children. ASD has many overlapping symptoms with other disorders and a better understanding of gesture use by children with ASD in comparison to non-typically developing children has the potential to aid in differential diagnosis. Moreover, for comparison of findings across studies and for research to be translated into clinical practice, there is a need for more consistent gesture terminology. Finally, while the present study adds novel information to the literature, the articles included in this study were published prior to 2014. Future scoping reviews, systematic reviews, and meta-analyses are needed to confirm the findings of this study and include more recent data.
CONCLUSION
There is a need for identification of diagnostic markers of ASD at younger ages [ 6]. This scoping review explored type and frequency of gesture use in children with ASD in comparison to other populations with the intent guide future studies and programs targeting early identification of ASD. The results of this study found that research has supported children with ASD as using different types and frequencies of gesture when compared to other populations suggesting that gestures can be used as an early diagnostic marker. The least studied age range of the articles included in this study was children under the age of 2 years. This shows the need for research in younger populations especially taking into consideration that the literature has supported early gesture use as an early indicator to detect ASD. Interestingly, the most studied age group was 4 to 5 years, which is consistent with the current average age of diagnosis of ASD. This raises the question whether the average age of diagnosis is so high because of this insufficient research in younger ages and supports Zwaigenbaum et al.’s assertion of the need for more early diagnostic markers [ 6]. This study also found that most frequently investigated comparison group was typically developing children. ASD is a disorder that has overlapping symptoms with many other disorders and if gestures are to be used as an early indicator of this disorder, more research is needed to include more diverse samples which will aid in differential identification and diagnosis. Finally, the terminology and definitions used for gesture were inconsistent across all studies. Standardization of terminology and associated definitions for various gesture types is necessary so that findings can be compared across studies and research can accurately be translated into clinical practice.
ACKNOWLEDGMENTS
The authors would like to thank all the researchers who have dedicated their time to exploring gesture use in children with ASD. We would also like to acknowledge the assistance of the following individuals involved in the data collection: Gayle Stewart, Monica Olmos, Arlene Nolasco, Hannah Vick, Jenna Grupo, and Patricia Simms.
Figure 1
Flow chart of scoping literature search. 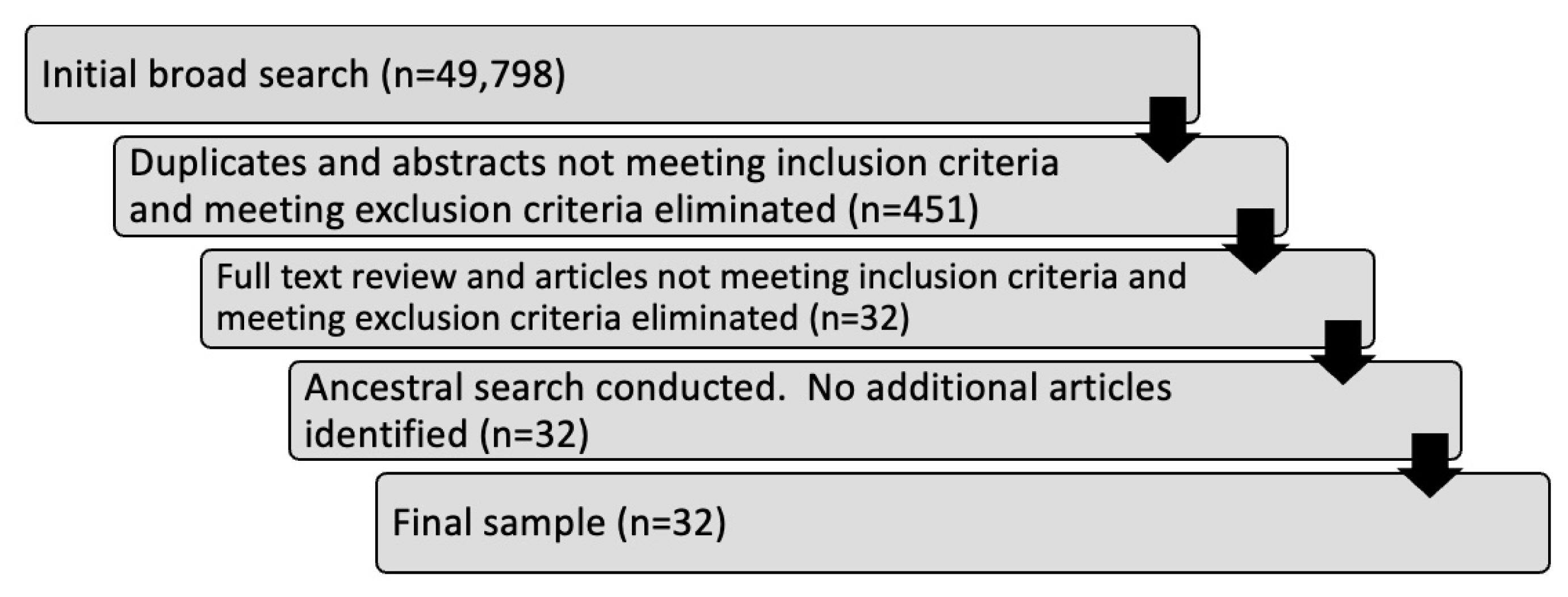
Table 1
Type of gesture use in children with asd in comparison to other populations
|
ASD Participant Age (In years) |
Comparison Group |
Significant Difference in Type |
Gesture Terminology |
Author |
|
0–1 |
1–2 |
2–3 |
3–4 |
4–5 |
5–6 |
6+ |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Prompted pointing Non-prompted pointing Atypical point.
|
Hobson et al., [21] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Social interaction gestures
|
Colgan et al., [20] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pointing Communicative Gestures Showing Use of another’s body to communicate Gestures Requesting Giving
|
Chawarska et al., [10] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nestling Anticipatory posture Social gestures Requesting gestures Joint Attention (Proto-declarative showing) Joint Attention (Proto-declarative pointing)
|
Clifford et al., [19] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Protoimperative pointing Protodeclarative pointing
|
Baron-Cohen [4] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Behavior regulation gestures Social Interaction Gestures Joint attention gestures
|
Watson et al., [10] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gestures Pointing Showing
|
Lincoln et al., [24] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gestures to initiate joint attention
|
MacDonald et al., [27] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Behavior regulation gestures
|
Maljaars et al., [28] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Communicative gestures Declarative gestures Imperative gestures
|
Carpenter et al., [14] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nonverbal Communication Pointing Reaching
|
Warreyn et al., [37] |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Landry & Loveland [23] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Early Developing gestures: touching taking More advanced gestures-pointing and showing
|
Loveland & Landry [26] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Declarative pointing gestures
|
Willemsen-Swinkels et al., [40] |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bishop et al., [13] |
Table 2
Frequency of gesture use in children with asd in comparison to other populations
|
ASD Participant Age (In Years) |
Comparison Group |
Frequency Results & Gesture Terminology |
Author |
|
0–1 |
1–2 |
2–3 |
3–4 |
4–5 |
5–6 |
6+ |
1 |
2 |
3 |
4 |
5 |
More |
Less |
No Diff. |
|
|
|
|
|
|
|
|
|
|
|
|
Atypical point*
|
|
Non-verbal deixis |
Hobson et al., [21] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Shows object*, point*
|
|
Mars et al., [29] |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Point, reach |
Charman et al., [15] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gestural joint attention*, initiates requests*, points for request*, brings for request*
|
|
Clifford & Dissanyke et al., [18] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pointing, vague pointing, show |
|
Osterling & Dawson [31] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gestures*
|
Gestures |
Osterling et al., [32] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Inventory of conventional gestures*
|
|
Wetherby et al., [39] |
|
|
|
|
|
|
|
|
|
|
|
|
Reach after tickle*, reaches to toy*
|
Show*, points to toy out of reach*
|
Reach + eye contact/tickle, reach to quiet adult, initiates turn taking, point, show, reach, points to toy out of reach |
Mundy et al., [3] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Point*, Gives/Shows*, Gives for help*, Touch |
|
Sigman et al., [34] |
|
|
|
|
|
|
|
|
|
|
|
|
Social interaction, behavior regulation |
Social interaction, Behavior regulation*, joint attention |
|
Watson et al., [10] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Requests composite*
|
Requests composite |
Mundy et al., [30] |
|
|
|
|
|
|
|
|
|
|
|
|
Push object with hand |
Gestures*, point to object*, social interaction*, gestures indicating excitement/accomplishment, shrugging of shoulders, opening of hands to indicate ‘all gone’ and ‘here’, joint attention initiation, joint attention response, representational gestures |
Behavior regulation, joint attention, joint attention response gestures |
Toret & Acarlar [36] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nonverbal communicative acts*, low level requests*, high level requests*, proximal point*
|
Initiating requesting high level, Low level requests |
Chiang et al., [17] |
|
|
|
|
|
|
|
|
|
|
|
|
Behavior regulation gestures*
|
|
|
Maljaars et al., [28] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Total hand gestures*, total head gestures*, all gestures*
|
|
Pendersen & Schelde [33] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pointing |
|
Warreyn et al., [38] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nonverbal communication*
|
Pointing |
Warreyn et al., [37] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Joint attention-structured setting*, Joint attention unstructured setting*, joint attention caregiving setting*
|
|
Wong & Kasari [41] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pointing*
|
Gestural behavior responses |
Landry & Loveland [23] |
|
|
|
|
|
|
|
|
|
|
|
|
Pointing*
|
|
Gestural joint attention behaviors, showing |
Loveland & Landry [26] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gesture*
|
|
Loveland et al., [25] |
|
|
|
|
|
|
|
|
|
|
|
|
Manipulate hand*
|
Contact point*, distal point*, show object*
|
Reach, give object, and touch object |
Stone et al., [35] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Coordinating gestures |
|
Kimhi & Bauminger-Zviely [22] |
Table 3
Significant findings for frequency of gesture use in children with asd in comparison to other populations
|
ASD Participant Age (In Years) |
Comparison Group |
Frequency Results & Gesture Terminology |
Author |
|
0–1 |
1–2 |
2–3 |
3–4 |
4–5 |
5–6 |
6+ |
1 |
2 |
3 |
4 |
5 |
More |
Less |
|
|
|
|
|
|
|
|
|
|
|
|
Atypical point*
|
|
Hobson et al., [21] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Shows object*, point*
|
Mars et al., [29] |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Charman et al., [15] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gestural joint attention*, initiates requests*, points for request*, brings for request*
|
Clifford & Dissanyke et al., [18] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gestures*
|
Osterling et al., [32] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Inventory of conventional gestures*
|
Wetherby et al., [39] |
|
|
|
|
|
|
|
|
|
|
|
|
Reach after tickle*, reaches to toy*
|
Show*, points to toy out of reach*
|
Mundy et al., [3] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Point*, Gives/Shows*, Gives for help*
|
Sigman et al., [34] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Behavior regulation*
|
Watson et al., [10] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Requests composite*
|
Mundy et al., [30] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gestures*, point to object*, social interaction*
|
Toret & Acarlar [36] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nonverbal communicative acts*, low level requests*, high level requests*, proximal point*
|
Chiang et al., [17] |
|
|
|
|
|
|
|
|
|
|
|
|
Behavior regulation gestures*
|
|
Maljaars et al., [28] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Total hand gestures*, total head gestures*, all gestures*
|
Pendersen & Schelde [33] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nonverbal communication*
|
Warreyn et al., [37] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Joint attention-structured setting*, Joint attention unstructured setting*, joint attention caregiving setting*
|
Wong & Kasari [41] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pointing*
|
Landry & Loveland [23] |
|
|
|
|
|
|
|
|
|
|
|
|
Pointing*
|
|
Loveland & Landry [26] |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gesture*
|
Loveland et al., [25] |
|
|
|
|
|
|
|
|
|
|
|
|
Manipulate hand*
|
Contact point*, distal point*, show object*
|
Stone et al., [35] |
REFERENCES
2. Lord C, Risi S, Lambrecht L, Cook EH, Leventhal BL, DiLavore PC, et al. The Autism Diagnostic Observation Schedule-Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders. 2000;30:205–223.  3. Mundy P, Sigman M, Ungerer J, Sherman T. Defining the social deficits of autism: the contribution of non-verbal communication measures. Journal of Child Psychology and Psychiatry. 1986;27:657–669.  4. Baron-Cohen S. Perceptual role taking and protodeclarative pointing in autism. British Journal of Developmental Psychology. 1989;7:113–127. 5. Camaioni L, Perucchini P, Muratori F, Milone A. Brief report: A longitudinal examination of the communicative gesture deficit in young children with autism. Journal of Autism and Developmental Disorders. 1997;27:715–725. 7. Maenner MJ, Shaw KA, Baio J, Washington A, Patrick M, DiRenzo M, et al. Prevalence of Autism Spectrum Disorder among children aged 8 years. Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveillance Summaries. 2020;69:1–12.
10. Watson LR, Crais ER, Baranek GT, Dykstra JR, Wilson KP. Communicative gesture use in infants with and without autism: a retrospective home video study. American Journal of Speech-Language Pathology. 2013;22:25–39. 12. Cooper H. Research synthesis and meta-analysis: A step-by-step approach (Applied Social Research Methods). 4rd ed. Los Angeles, CA: Sage Publications, 2009.
13. Bishop S, Gahagan S, Lord C. Re-examining the core features of autism: a comparison of autism spectrum disorder and fetal alcohol spectrum disorder. Journal of Child Psychology and Psychiatry. 2007;48:1111–1121. 14. Carpenter M, Pennington BF, Rogers SJ. Interrelations among social-cognitive skills in young children with autism. Journal of Autism and Developmental Disorders. 2002;32:91–106. 15. Charman T, Swettenham J, Baron-Cohen S, Cox A, Baird G, Drew A. An experimental investigation of social-cognitive abilities in infants with autism: clinical implications. Infant Mental Health Journal. 1998;19:260–275. 16. Chawarska K, Klin A, Paul R, Volkmar F. Autism spectrum disorder in the second year: stability and change in syndrome expression. Journal of Child Psychology and Psychiatry. 2007;48:128–138. 20. Colgan SE, Lanter E, McComish C, Watson LR, Crais ER, Baranek GT. Analysis of social interaction gestures in infants with autism. Child Neuropsychology. 2006;12:307–319. 21. Hobson RP, Garcia-Perez RM, Lee A. Person-centered (deictic) expressions and autism. Journal of Autism and Developmental Disorders. 2010;40:403–415. 23. Landry SH, Loveland KA. Communication behaviors in autism and developmental language delay. Journal of Child Psychology and Psychiatry. 1988;29:621–634. 24. Lincoln AJ, Searcy YM, Jones W, Lord C. Social interaction behaviors discriminate young children with autism and Williams syndrome. Journal of American Academy of Child and Adolescent Psychiatry. 2007;46:323–331. 25. Loveland KA, Landry SH, Hughes SO, Hall SK, McEvoy RE. Speech acts and the pragmatic deficits of autism. Journal of Speech and Hearing Research. 1988;31:593–604. 27. MacDonald R, Anderson J, Dube WV, Geckeler A, Green G, Holcomb W, et al. Behavioral assessment of joint attention: A methodological report. Research in Developmental Disabilities. 2006;27:138–150. 28. Maljaars J, Noens I, Jansen R, Scholte E, van Breckelaer-Onnes I. Intentional communication in nonverbal and verbal low-functioning children with autism. Journal of Communication Disorders. 2011;44:601–614. 29. Mars AE, Mauk JE, Dowrick PW. Symptoms of pervasive developmental disorders as observed in prediagnostic home videos of infants and toddlers. The Journal of Pediatrics. 1998;132:500–504. 32. Osterling JA, Dawson G, Munson JA. Early recognition of 1-year-old infants with autism spectrum disorder versus mental retardation. Development and Psychopathology. 2002;14:239–251. 34. Sigman M, Mundy P, Sherman T, Ungere J. Social interactions of autistic, mentally retarded, and normal children and their caregivers. Journal of Child Psychology and Psychiatry. 1986;27:647–656. 35. Stone W, Ousley O, Yoder P, Hogan K, Hepburn S. Nonverbal communication in two- and three-year old children with autism. Journal of Autism and Developmental Disorders. 1997;27:677–696. 36. Toret G, Acarlar F. Gestures in prelinguistic Turkish children with autism, down syndrome, and typically developing children. Educational Sciences: Theory & Practice. 2011;11:1471–1478.
40. Wilemsen-Swinkels SHN, Buitelaar JK, Weijen FG, van Engeland H. Timing of social gaze behavior in children with pervasive developmental disorder. Journal of Autism and Developmental Disorders. 1998;28:199–210.
|
|











