Effective Duration of Auditory Training for Speech Perception in Hearing-Impaired Listeners: A Systematic Review and Meta-Analysis
Article information
Abstract
Purpose
The purpose of this study was to conduct a meta-analysis to determine the effective duration of auditory training for hearing aid users and cochlear implant users and to identify factors that influence the effectiveness of auditory training.
Methods
We searched literature published from January 1996 to August 2021 in Pubmed, Web of Science, Embase and Cochrane Library. A total of 24 studies that met the selection criteria were systematically reviewed and analyzed through meta-analysis. Standardized mean differences and 95% confidence intervals were calculated.
Results
The overall meta-analysis results for auditory training showed an effect size of −0.833, and the effect size was larger in “more than 600 minutes of auditory training” compared to “less than 600 minutes”. There was no statistically significant difference in effect size during follow-up observation after the completion of auditory training, with an effect size of 0.057 (95% CI: −0.113–0.112, p=0.988). Subgroup analysis showed that the effect size was larger in the “children” group than in the “adult” group. The effect size of auditory training was larger when the auditory training and measurement conditions were the same.
Conclusions
Auditory training can improve speech perception in individuals wearing HA and/or CI, and the training effect was shown to be maintained even after the completion of auditory training. In addition, it was found that the longer the duration of auditory training (more than 10 hours), the greater the training effect.
INTRODUCTION
Approximately 500 million people globally have hearing loss, and this number is expected to increase with the aging population [64]. The World Health Organization [65] reported that more than 430 million people worldwide need rehabilitation to address their hearing loss. It is predicted that more than 700 million people will have hearing loss in 2050 [65]. Hearing loss can negatively affect daily functions and quality of life, causing cognitive and functional deterioration, social isolation, increased risk of fall, and reduced social and emotional function [12,31,35].
The use of hearing aid (HA) and cochlear implant (CI) is the most common method for restoring the hearing of the hearing-impaired. However, it is difficult to expect an improvement in communication ability solely through the use of HA and CI. Despite using such amplifiers, hearing-impaired individuals face communication difficulties every day, especially in environments that are not ideal for communication, such as noisy environments [21,29]. HA and CI mount various technologies to enhance communication in noisy environments. For example, noise reduction and directional microphones are technologies that reduce noise and emphasize sound, but communication in noisy environments remains a challenging task for hearing-impaired individuals [53,66]. Many researchers [1,36,43] have reported that hearing-impaired individuals continue to face communication difficulties even with the use of amplifiers due to the decline in their cognitive abilities, such as working memory, executive function, and attention.
One way to improve the cognitive abilities of the hearing-impaired is through auditory training. Auditory training involves actively listening to sounds and has been shown to be effective in many studies. Auditory training can be divided into two approaches: the bottom-up approach, which involves training to discriminate speech sounds, and the top-down approach, which involves training to comprehend the content of sentences. Many researchers report that both approaches result in neural plasticity and increased communication ability [18,36,42]. Neural plasticity can occur when an individual acquires new knowledge/skills through training, resulting in the growth of neural pathways, the creation of new circuits, and the formation of synapses between neurons. Additionally, auditory training can lead to positive effects such as increased satisfaction with hearing aid use and improved quality of life [10,27,68].
To demonstrate the effectiveness of auditory training, two factors must be confirmed. The first is the ‘transfer of learning,’ which means that the performance should improve not only in the trained tasks but also in untrained tasks. That is, auditory training can be considered effective if it improves communication skills in the real world. The second factor is the retention of the training effect. If the effect of the training disappears shortly after the training, it cannot be considered effective. Many studies have been conducted on the transfer of learning and retention of training effect in auditory training, but the optimal duration of training for achieving effective results is still unclear.
To our knowledge, no systematic review or meta-analysis has been published to provide data that focuses on improving speech perception for individuals with HA or CI by quantitatively integrating the results using statistical methods. Although Lawrence et al., [34] conducted a meta-analysis on the efficacy of auditory training for hearing impairment, their focus was on cognitive function. In this meta-analysis, we aimed to calculate the overall effect size of efficacy on speech perception for HA or CI users and identify the effective training duration, including methodology of the auditory training.
The primary aim of this systematic review and meta-analysis is to examine the effectiveness of the most effective auditory training period for hearing aid users or cochlear implant users. The secondary goals are to (i) examine the retention of training-related improvement and (ii) investigate factors affecting training outcomes.
METHODS
All the processes, including inclusion criteria, exclusion criteria, article search strategy, and article selection, followed a Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols (PRISMA-P) statement [41].
Search strategy
The search was performed to find published articles on improving speech perception after auditory training of hearing-impaired listeners with HA or CI.
The search was conducted using the same keywords suggested by [19], including “hearing loss” OR “cochlear implant” OR “hearing aid” OR “hearing impair*” AND “auditory training” OR “auditory learning” OR “perceptual training” OR “perceptual learning” AND “speech perception,” The search was conducted on four databases, namely PubMed, Web of Science, Embase, and Cochrane Library. The search was included articles published from January 1996 to August 2021. Only original articles were included, while proceedings, book reviews, conference abstracts, and review studies were excluded. Sweetow & Sabes [60]did review seven papers on the auditory training, and they studied the papers published before 1996. Thus, the articles that have been included in this study have been published from January 1996 to August 2021.
Article selection
For the homogeneity and reliability of the eligible studies, a strategy of Participants, Intervention, Control, Outcomes, and Study design (PICOS) was applied. The PICOS criteria used in this study are displayed in Table 1.
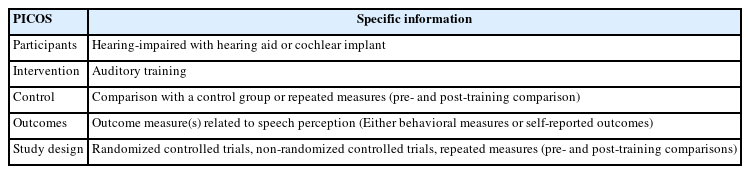
Inclusion criteria for the current study based on Participants, Intervention, Control, Outcomes, and Study designs (PICOS)
A total of 6,105 records were searched using four electronic journal databases. After removing duplicate articles, a total of 5,756 articles remained. Then, the following criteria were used to screen for eligibility. After first screening the titles and abstracts, 5,330 articles were excluded from the full-text assessment. The full texts of the remaining 426 articles were then examined for inclusion based on the PICOS criteria and relevance. In the evaluation process, two researchers assessed the eligibility of identified studies independently. The articles were again reviewed and discussed if the two researchers did not agree.
Three hundred fifty-eight papers were excluded based on PICOS criteria, and 68 remained. In the process of data extraction, a total of 44 studies that had no standard deviation data (n=31), no specific data presented (n=10), and mixed data of participants (n=3) were excluded. Finally, 24 articles met the PICOS criteria for this study. The flow of articles and screening procedure is shown in Figure 1.
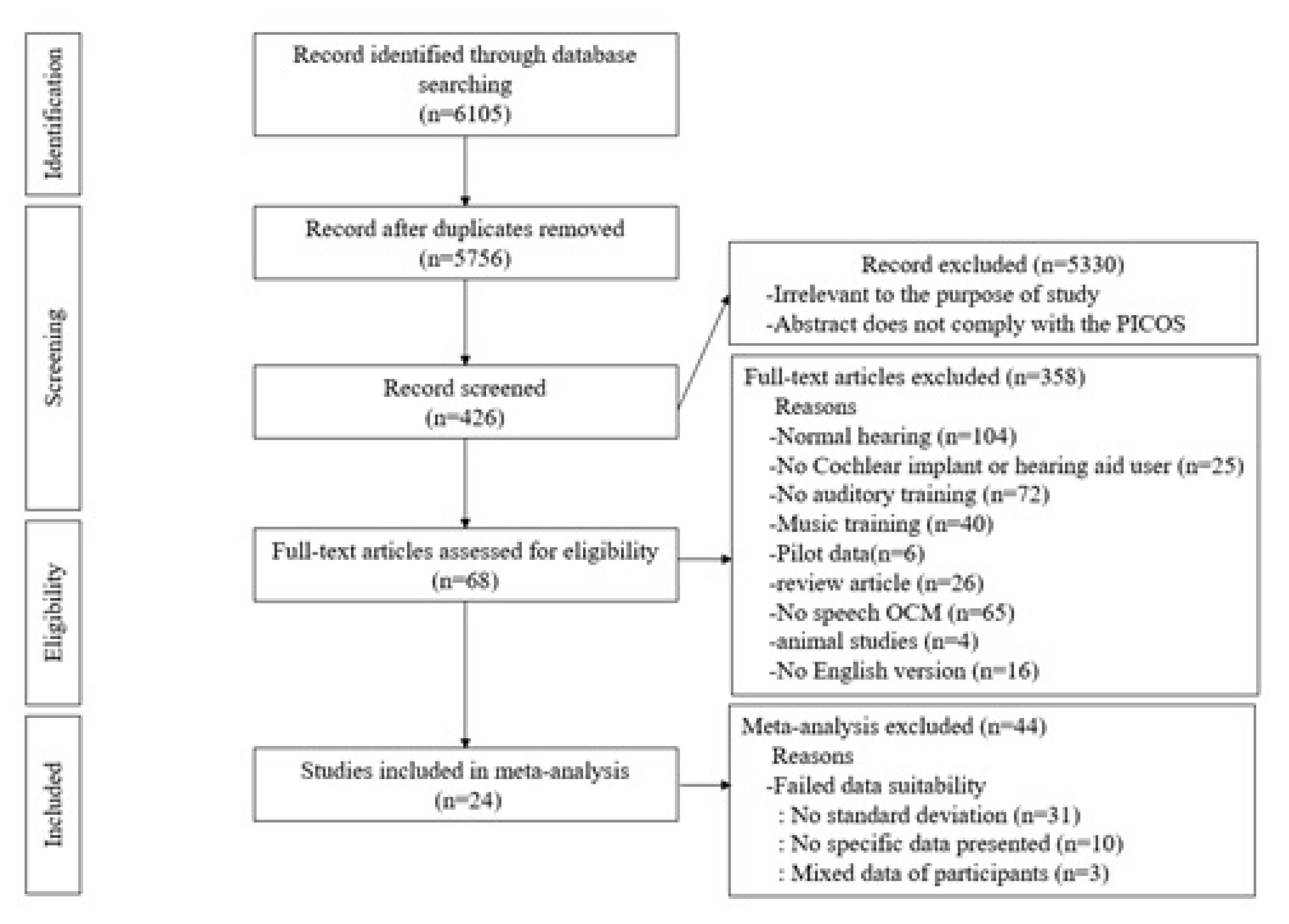
PRISMA flow diagram. PICOS, Participants, Intervention, Control, Outcomes, Study Designs; OCM, outcome measure; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study quality and potential sources of study bias
The Physiotherapy Evidence Database (PEDro) scale [5] evaluated the study quality and any potential sources of study bias. The PEDro scale is composed of 11-items aimed for rating the methodological quality of Randomized Controlled Trials (RCTs). A total of 11 questions were used to evaluate the quality of RCTs on two aspects, including internal validity (criteria 2–9) and sufficient statistical information to make it interpretable (criteria 10 and 11), and shown in Table 2. The risk of bias for each item was rated as “yes” or “no.” “Yes” indicated a low risk of bias, and “no” showed a high risk of bias. Each item was assigned 1 for “yes” or 0 for “no.”
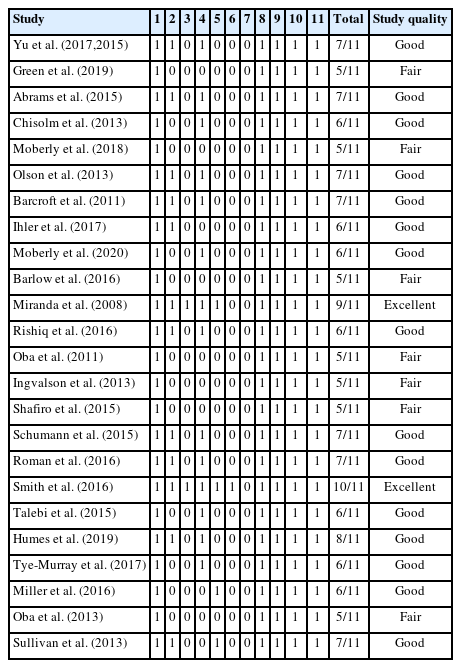
List of quality assessment of study by PEDro scale
A grade of studies with PEDro scores ranging from 9 to 11 was of “excellent” quality, 6 to 8 was supposed to be of “good” quality, while studies scoring 4 or 5 were of “fair” quality, and below four were of “poor” quality. Two investigators independently assessed the 24 studies using the PEDro scale.
Meta-analysis
We obtained the following information for the meta-analysis: author, year of publication, participant characteristics (number, age, and hearing device), intervention details (auditory training duration and condition), control group details (number, age, and hearing aid/CI use), study design, and outcome measures (measurement condition, unit, and follow-up duration). The Comprehensive Meta-Analysis software (Ver. 3, Biostat Inc., Englewood, NJ, USA) were used for all analyses. For the analysis, the 24 articles included speech perception results of pre-and post-auditory training, appropriate outcome measures, and auditory training. The effect size was calculated using sample size, mean, and standard deviation of pre-and post-training outcomes. The effect size was also calculated as the standard mean difference (SMD) because the characteristics of the qualitatively synthesized data from the included articles were continuous, and the types of outcome measures were different. Negative effect size indicates greater effectiveness of auditory training. The effect size of the standard mean difference was considered as −0.2 for small, −0.5 for moderate, and −0.8 for high [9].
The estimate the pooled effect of auditory training on each outcome measure, we used the random-effect model. We analyzed the data according to the total training duration to investigate the effective duration of auditory training, which we divided into two groups: short (<600 minutes) and long (≥600 minutes) durations.
When we extracted multiple outcome results from one study, we considered individual data and performed separate analyses. For example, we treated each result as separate data when evaluating auditory training effectiveness with different outcome measurements. We also considered measurements taken during and after training in the same subject as independent data.
To conduct subgroup analysis, we divided subjects into adults (18 years of age and older) and children (below 18 years of age) based on their age, and hearing devices into HA and CI (including bimodal users) based on the type of device used. We also investigated effective training conditions by dividing them into “in noise” or “in quiet”.
To evaluate publication bias, we sued a funnel plot and Egger’s regression test, as well as Rosenthal’s classic fail-safe N. Specifically, we considered publication bias not to be an issue if the fail-sage N value was greater than the “5×number of studies (k)+10” that contributed to each analysis.
Heterogeneity and subgroup analysis
The quantitative exploration of variance heterogeneity across the included studies involved the use of Cochrane’s Q and Higgins I2-statistic values. A Q-test p-value of less than 0.10 was considered present. The I2-values were used to measure the proportion of observed variance between trials in individual studies due to real differentials in effect size. These values were presented as a percentage ranging from 0 to 100. Heterogeneity was regarded as low if the I2-value was below 25%, moderate if it was between 25–75%, and high if it was between 75–100% [20].
The statistical significance at a 95% CI indicated the presence of heterogeneity across the dataset of articles.
To further analyze the heterogeneity, a subgroup analysis was performed, with planned variables including (1) the age of the participants and (2) the auditory training condition. The significance of the findings, heterogeneity between subgroups, and study’s effect size were also compared.
Sensitivity analysis
A sensitivity analysis was conducted to determine the impact of excluding each study on the overall results.
RESULTS
Quality assessment of study
PEDro scores were received by the articles reviewed in this study (Table 2).
Twenty-four of the two studies were ranked as “excellent,” with total values of 9 to 11 [13,56]. The 15 studies were evaluated as “good,” with scores between 6 and 8 [2,3,7,22,23,37,39,45,49, 50,54,58,61,62,67]. The remaining seven studies [4,17,24,40,43, 44,55] were assessed as “fair,” with scores between 4 and 5. The overall methodological quality was acceptable (total mean score=6.4, SD=1.3, range 5–10).
Characteristics of the study
The characteristics of included studies are shown in Table 3. Data extracted from the 24 studies are presented in the PICOS criteria.
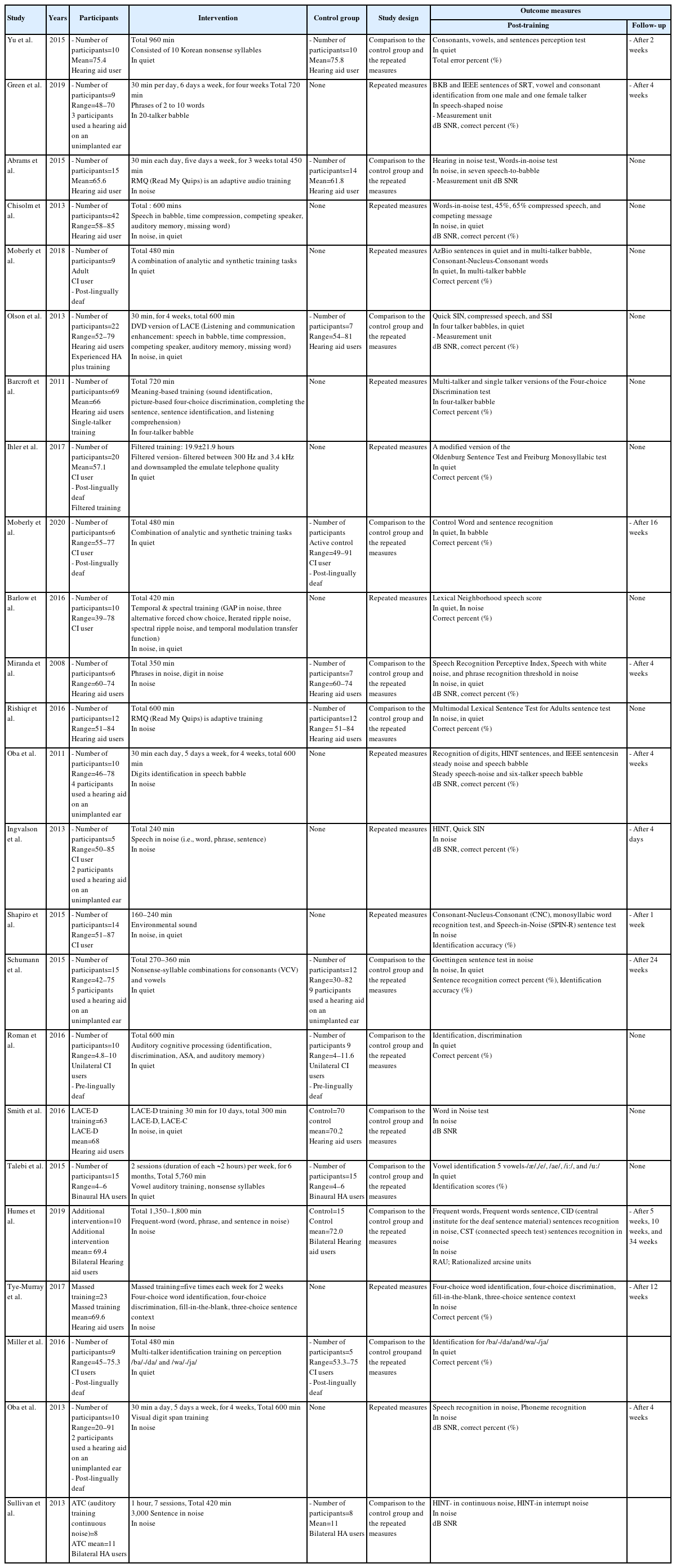
Characteristics for all enrolled studies for the participants, the intervention, control group, and the outcome measures
Participants
All participants included in the studies had hearing impairment and were using either hearing aids or cochlear implants. Among the twelve studies, only hearing aid users were included [2,3,7,13,22,45,49,56,58,61,62,67], while in seven studies, only cochlear implant users were included [4,23,37,39, 40,50,55]. Five studies included both cochlear implant and bimodal users [17,24,43,44,54]. The majority of the studies were conducted with adults, while only three studies included children as participants [50,58,61].
Intervention
The intervention analyzed in the study was auditory training, which varied in duration and condition across the included studies. Training duration was classified as short (<600 minutes) or long (≥600 minutes). Ten studies had a training duration of less than 600 minutes [2,4,13,24,37,39,40,54,55,58], while 11 studies had a complete training duration of more than 600 minutes [3,8,17,22,23,44,49,50,61,62,67]. Three studies had a total training time of both less than 600 minutes and more than 600 minutes [43,45,56]. The training condition was not standardized across studies.
The conditions for auditory training were categorized as “in quiet” and “in noise”. Eleven studies conducted auditory training under “in noise” conditions [2,3,13,17,22,24,43,44,49,58,62], while eight studies conducted auditory training under “in quiet” conditions [23,37,39,40,50,54,61,67]. Five studies completed auditory training under both “in noise” and “in quiet” conditions [4,7,24,43,44,45,55,56,62].
Controls
Of the 24 articles, 13 studies included a control group consisting of individuals with hearing loss who used hearing aids or cochlear implants [2,13,22,45,67,37,39,49,50,54,56,58,61]. The remaining 11 studies employed repeated measures for pre- and post-training comparison [3,4,7,17,23,40].
Outcome
All studies evaluated speech perception outcomes, including syllables, words, and sentences. In ten studies, speech perception was measured in noisy conditions such as multi-talker babble and steady speech-noise [3,17,22,24,43,44,55,56,58,62]. In five studies, speech perception was measured in quiet conditions [23,37,50,61,67]. Nine studies measured speech perception outcomes in both quiet and noisy conditions [2,4,7,39, 40,45,49,54].
Follow up
To confirm the maintenance of training effects, eleven studies were followed up [13,17,24,39,43,44,54,55,62,67].
Study design
All 24 studies included repeated measures, while 13 of them used control groups for comparison [2,13,22,37,39,45,49,50,53,56,58,61,67].
Overall results of auditory training effects
The effect sizes for the studies using the random-effects model are presented in Figure 2. SMD were used to analyze data with mean and SD to consider the dataset’s characteristics. The results showed a significant improvement in speech perception after auditory training (SMDs −0.833, 95% CI: −0.960~−0.707, p=0.000), as depicted in Figure 3 which displays the funnel plot. We conducted Egger’s regression analysis, which revealed evidence of publication bias (Intercept: −2.92, 95% CI: −3.74~−2.07, p=0.000). However, the fail-safe N analysis using Rosenthal’s [51] method suggested that 8,790 studies with zero-effect would be needed to render the mean effect size of auditory training nonsignificant. Therefore, publication bias was unlikely to interfere with the main results of this meta-analysis. The Higgins I2-statistics and Cochran’s Q-test indicated a moderate level of heterogeneity (I2: 70.12%, Q: 478.65, p=0.000).
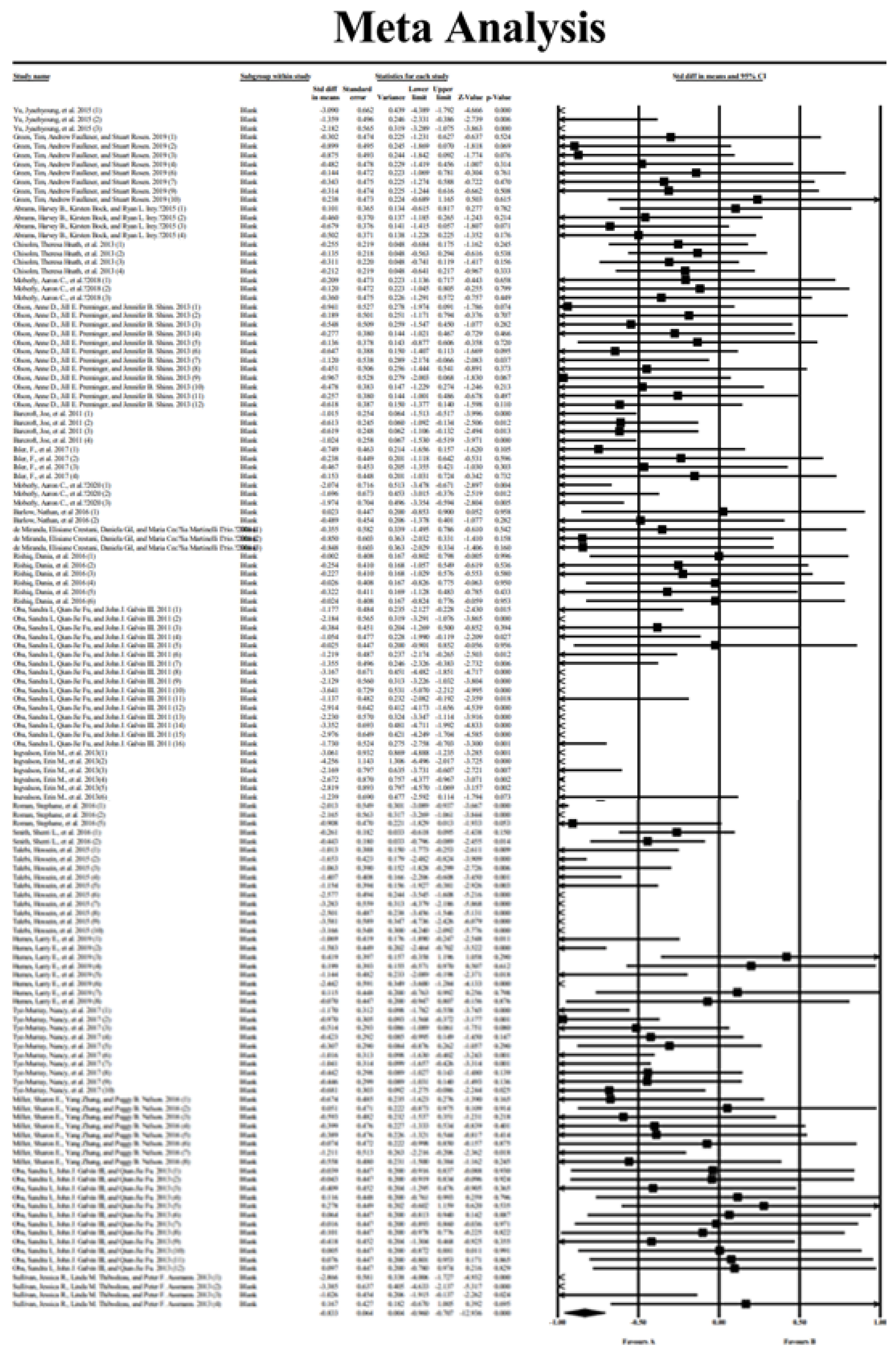
Forest plot of auditory training effects. Including 24 studies.
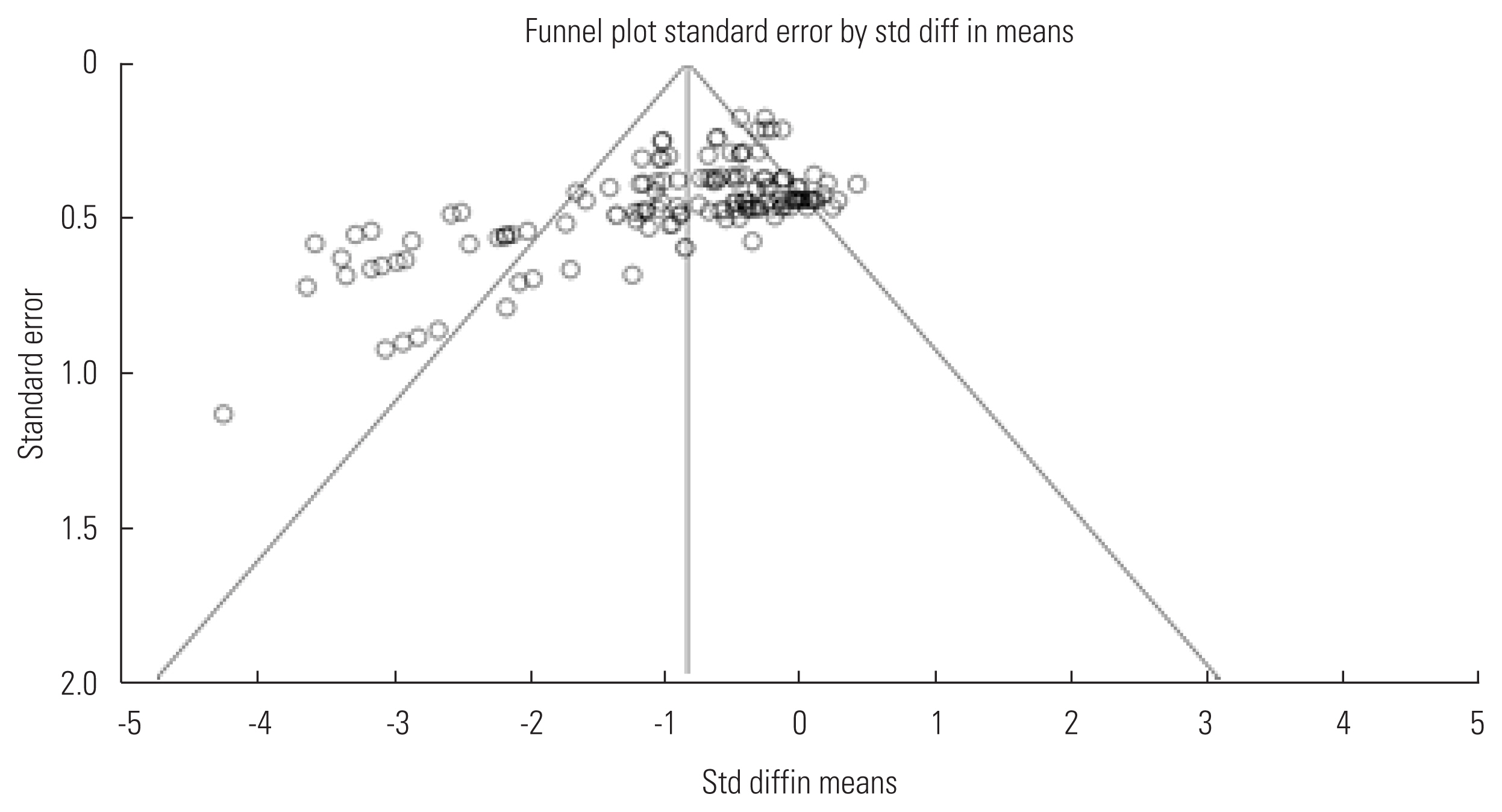
Funnel plot for publication bias of auditory training effects. including 24 studies.
Efficacy duration of the auditory training
To analyze the effect of auditory training duration, we divided the duration into two groups: ‘Short’ (<600 minutes) and ‘Long’ (≥600 minutes), as shown in Figure 4. The effect size for the ‘Short’ group was −0.747 (95% CI: −0.932~−0.562), while the effect size for the ‘Long’ group was −0.890 (95% CI: −1.061~−0.719). As demonstrated, the effect size of the ‘Long’ group was larger than that of the ‘Short’ group.

Meta-analysis according to the training duration.
Training retention
Retention of auditory training was defined as a non-significant decrease in post-training performance at a delayed post-training follow-up assessment. Such follow-up assessments were reported in 11 studies, ranging from 4 days to 34 months after post-training. Figure 5 displays the effect size at follow-up, which was 0.057 (95% CI: −0.113~0.112, p=0.988).

Meta-analysis according to the training retention.
Subgroup analysis
The meta-analysis conducted a subgroup analysis based on age and training conditions.
Age
The effect sizes for the ‘Adult’ and ‘Children’ groups were −0.674 (95% CI: −0.789~−0.559) and −1.915 (95% CI: −2.410~−1.420), respectively, as shown in Figure 6. The effect size for the ‘Children’ group was significantly larger than that for the ‘Adult’ group.

Meta-analysis according to the age.
Training condition
Due to the small number of studies for the ‘children’ group, the subgroup analysis of training conditions was only conducted for the ‘adult’ group. The ‘Training in quiet’ group had effect sizes of −0.784 (95% CI: −1.050~−0.518) and −0.560 (95% CI: −1.054~−0.066) in the ‘in quiet’ and ‘in noise’ tests, respectively. The ‘Training in noise’ group had effect sizes of −0.233 (95% CI: −0.412~−0.053) and −0.757 (95% CI: −0.908~−0.606) in the ‘in quiet’ and ‘in noise’ tests, respectively. Notably, the effect size of the outcome measurement performed in the ‘in noise’ condition was significantly larger than that in the ‘in quiet’ condition for the ‘Training in noise’ group. Conversely, for the ‘Training in quiet’ group, the effect size was significantly larger in the ‘in quiet’ condition than in the ‘in noise’ condition.
Sensitivity analysis
The sensitivity analysis revealed that the exclusion of any individual study did not have a significant impact on the overall pooled effect size.
DISCUSSION
This study examined the efficacy of auditory training on speech perception in individuals with hearing loss who use hearing aids, cochlear implants, or both. The results showed that auditory training was effective in improving speech perception in this population. A total of 24 studies [2,3,4,7,13,17,22–24,37,39,40,43–45,49,50,54–56,58,61,62,67] were included in this meta-analysis, and significant improvements in speech perception were observed in the individuals who underwent auditory training.
These meta-analysis results confirm previous findings that auditory training is more effective than no intervention for improving speech perception in individuals with hearing loss, which is consistent with the findings of several studies [7,15,19,28,45,47,63]. The following sections discuss the research questions addressed by our study.
What is the most effective training duration for auditory training?
This study examined the impact of auditory training duration on speech perception improvement. The results revealed that both short-term and long-term auditory training interventions had a positive effect on speech perception improvement, and the training duration depended on the specific goals or purposes of the training [55,61]. The duration of auditory training used in the studies ranged from 160 to 5,760 minutes. The largest effect size was found for training periods longer than 600 minutes, compared to periods shorter than 600 minutes [3,7,17,22,23,44,49,50,61,62,67].
Therefore, we suggest that a longer training period (e.g., more than 600 minutes) can optimize the effectiveness of a rehabilitation program for individuals with hearing impairment. However, it is important to note that a short training duration in this study also provided a certain amount of improvement in speech perception [24,25,57].
Determining the retention of learning after auditory training is a crucial indicator of its benefits [19]. Previous studies have measured the retention of improved performance by comparing subjects’ performance at baseline to their performance after completion of training [14,30,38,48].
In this study, we analyzed 11 out of 24 studies that included follow-up evaluations ranging from 4 days post-training [24] to 34 months [22]. Our analysis showed that auditory training benefits appeared to have been maintained with a non-significant decrease in performance when comparing post-training and follow-up assessments. These results suggest that auditory training may provide lasting benefits beyond any naturally occurring learning effects.
Does auditory training affect adults and children differently?
To investigate whether the benefits of auditory training differ between “adults (>18 years of age)” and “children (<18 years of age)”, we conducted a subgroup analysis of the included studies. Our analysis revealed that auditory training had a significant positive effect on speech perception in both adult and child populations. Specifically, in adults, a medium effect size was found, whereas in children, a large effect size was observed [8,22,24,49,50,61,62].
Auditory training has been shown to induce anatomical and functional neuroplasticity in children [52]. Based on the principle of neuroplasticity, it is plausible that children who wear hearing aids or cochlear implants may benefit more than adults [16].
In addition to age, it would have been desirable to examine the effect of hearing aids versus cochlear implants in this study. However, most of the children in the study used cochlear implants, and the limited data precluded further subdivision of participants based on hearing aid use or cochlear implant use.
What is the most effective condition for auditory training?
Auditory training has been shown to improve speech recognition in noise conditions for individuals with hearing loss [6,59], including children with hearing loss [58], and cochlear implant users in noisy environments [14].
The results of this study indicate that the “in quiet” training group had a higher effect size in the “in quiet” condition than in the “in noise” condition, whereas the “in noise” training group had a higher effect size in the “in noise” condition than in the “in quiet” condition. This finding suggests that the training effect is stronger when the training and measurement conditions match. However, even when auditory training was conducted in both quiet and noise conditions, speech perception improved in both conditions.