Discriminative and predictive ability for screening the Korean dysphonic patients using self-reported questionnaires
Article information
Abstract
Purpose
The purpose of this study was to verify the discriminative and predictive abilities of the Korean versions of the Voice Handicap Index (K-VHI), Voice-Related Quality of Life (K-VRQOL), and Voice Catastrophization Index (K-VCI) for dysphonia screening.
Methods
A total of 132 and 244 subjects in the control and case groups, respectively, completed the K-VHI, K-VRQOL, and K-VCI. Using the different types of questionnaires, we tried to verify whether age, symptom duration, type of diagnosis, and gender affected the results, and analyzed the cut-off points for screening dysphonic patients.
Results
The mean scores of questionnaires were not affected by factors such as age, symptom duration, type of diagnosis, or gender. All questionnaires showed a significant correlation with one another. The mean K-VHI and K-VCI scores of the case group were significantly higher than those of the control group. The mean K-VRQOL score of the case group was significantly lower than that of the control group. The cut-off points for the K-VHI, K-VRQOL, and K-VCI were 12.1, 91, and 6.1, respectively. The data showed relatively high sensitivity, specificity, and area under the curve values at each cut-off point (above 0.9), indicating excellent accuracy and a high power of discrimination.
Conclusions
The cut-off points identified in our study for the K-VHI, K-VRQOL, and K-VCI for distinguishing patients with voice disorders from the control group can be used as criteria to screen for Korean dysphonic patients.
INTRODUCTION
Voice disorders impair patients’ quality of life (QOL) [1]. Various voice evaluation tools have been introduced and used; of these, self-reported questionnaires on voice disorders provide insights into why patients with similar voice disorders experience different levels of QOL-related decrements and thus, assess the impact of voice disorders on QOL [2–5]. Patients with dysphonia may lose time from work, seek disability claims, and utilize health care resources, thus exacerbating societal economic hardships and decreasing productivity [1]. Considering these problems, it is essential to determine the complete impact resulting from the disability in patients with voice disorders [6,7]. A number of self-reported questionnaires have been developed, including, the Voice Handicap Index (VHI) [5], the VHI-10 [8], and the Voice-Related Quality of Life (VRQOL) [9]. The VHI and VRQOL are reported to valid tools to assess the QOL and have been translated into multiple languages [10–17].
Recently, there have been many studies on the effects of speech problems on catastrophization and QOL, as well as the relationship among them [18]. Catastrophization is a phenomenon of cognitive distortion frequently associated with anxiety and depressive disorders, and is characterized by concern, fear, and inability to divert attention from pain [19,20]. It relates to the patients’ inner world, thoughts, and beliefs; whereas QOL relates to the outer world and general well-being in different aspects of life, including environmental inter actions. More specifically, catastrophization is distinct from QOL, handicap, or disability which relates to aspects of the patient’s outer life. Patients with voice disorders were found to have a higher prevalence of depression, anxiety, personality, and other psychiatric disorders [18,21–23]. Although the concepts of QOL and catastrophization may be different, individuals who catastrophize tend to have poorer QOL and higher levels of disability than those who do not [18]. Shoffel-Havakuk et al. developed the Voice Catastrophization Index (VCI) based on the Pain Catastrophizing Scale [18,24], and verified its validity and reliability for estimating catastrophization in patients with voice disorders.
Many studies report that the three questionnaires are valid tools [9,18,25]. However, the validity and reliability of self-reported questionnaires do not predict the accuracy of diagnosis, case identification, risky behaviors, the patients’ inner world (e.g., catastrophization), or QOL. Some studies have emphasized the diagnostic capability of the VHI in clinical practice and its ability to differentiate dysphonic from normal voices [5,6,26]. Other studies have evaluated self-reported questionnaires as a screening tool to identify dysphonic voices [27,28]. Contrary to studies which use the VHI and VRQOL, studies on the diagnostic capability of the VCI are lacking. Most importantly, there are no studies which analyze the diagnostic capability of the VCI in Korean dysphonic patients. Combined, the diagnostic capability of the three questionnaires is able to verify the effect of a voice disorder on a patient’s outer (QOL) and inner (catastrophization) life.
In terms of the diagnostic capabilities of self-reported questionnaires, it is important to analyze their sensitivity (the proportion of patients with the disease who have a positive test), specificity (the proportion of patients without the disease who have a negative test), and the cut-off point for differentiating dysphonic from normal voice. In the present study, we evaluated and compared three questionnaires (K-VHI, K-VRQOL, and K-VCI) to [1] determine the cut-off points at which the tests differentiate dysphonic from normal voice; and [2] determine the diagnostic capability of the three questionnaires for Korean patients.
METHODS
Patients
The present study was approved by the Institutional Review Board of Pusan National University Hospital. A total of 403 patients who visited the Pusan National University Hospital laryngology clinic, in South Korea between January 2019 and August 2019 were selected. All diagnoses were made by one otolaryngologist and one speech language pathologist using laryngoendoscopy. Patients who could not complete the required questionnaires and patients with a psychiatric history were excluded.
Based on these exclusion criteria, a total of 376 patients were included in this study and all of them could complete the required questionnaires independently. Next, the patients were classified into two groups: the control group and the case group. The control group (n=132) included all new patients with swallowing problems (foreign bodies in the larynx, coughing, and chocking when eating or drinking), tonsillitis, adenoid hypertrophy, and cough (without voice complaints). The case group (n=244) included all new patients with either clinically perceived dysphonia or a patient-reported voice complaint. All patient information is included in Table 1. There was no significant difference in the age (p value=0.875) or in the gender ratio between the two groups (p value=0.713).
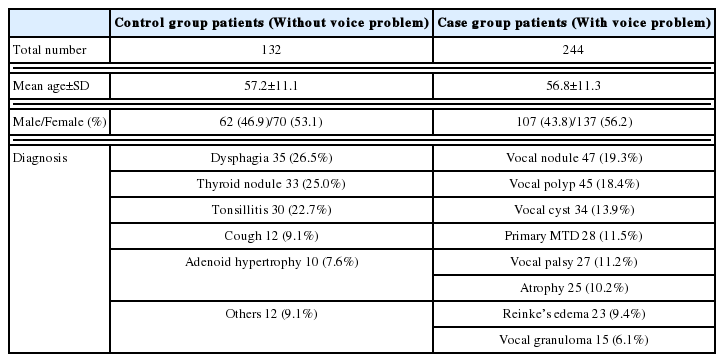
The information on patients
Study design
The Korean version of the VHI (K-VHI) [10], VRQOL (K-VRQOL) [29], and VCI (K-VCI) [25] were used and all patients completed these questionnaires at the initial visit.
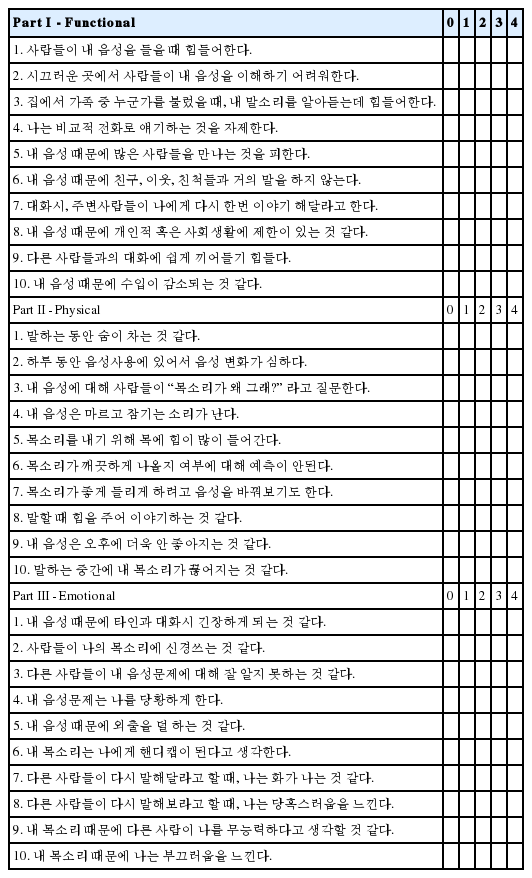
The K-VHI included 30 items, divided into three subtypes: functional, physical, and emotional. For each item, the patient was asked to indicate severe degrees of thoughts and feelings on a five-point numerical scale (0=not at all; 1=to a slight degree; 2=to a moderate degree; 3=to a great degree; 4=all the time). The maximal possible score is 120, and the minimal score is 0; a high score indicates a high severe degree of voice disorder. The K-VHI questionnaire is presented in Appendix A.
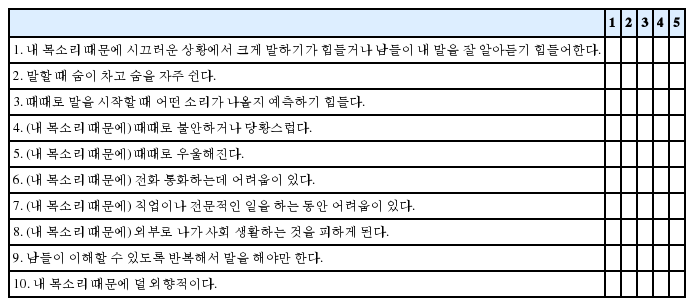
The K-VRQOL include 10 items; for each item, the patient was asked to indicate how severe their thoughts and feelings were on a five-point numerical scale (1=not at all; 2=to a slight degree; 3=to a moderate degree; 4=to a great degree; 5=all the time). The standard score for the K-VRQOL was calculated using the following formula [29]:
The maximum possible score is 100 (good V-RQOL), and the minimum possible score is 0 (poor V-RQOL). The K-VRQOL questionnaire is presented in Appendix B.
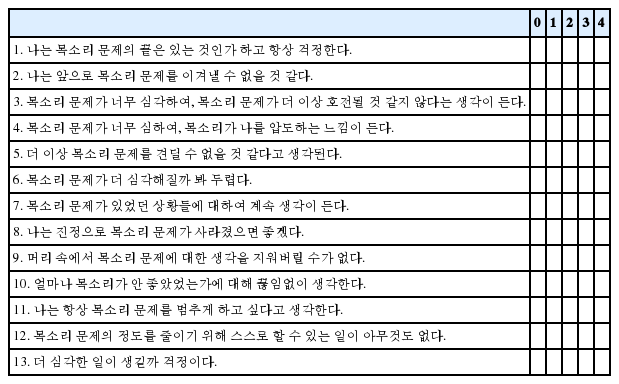
The K-VCI include 13 items, divided into three dimensions: rumination, magnification, and helplessness. Rumination (items 8–11) involves how consumed the patient’s thoughts are by their symptoms. Magnification (items 6, 7, and 13) indicates exaggeration of the impacts of their symptoms and thoughts about a much poorer prognosis. Helplessness (items 1–5 and 12) involves feeling that nothing will ever improve their situation. For each item, patients were asked to indicate severe degrees of their thoughts and feelings using a five-point numerical scale (0=not at all; 1=to a slight degree; 2=to a moderate degree; 3=to a great degree; 4=all the time). The maximum possible score is 52, and the minimum possible score is 0; a higher score represents higher levels of catastrophization of the voice condition [18]. The K-VCI questionnaire is presented in Appendix C.
Statistical analyses
The Statistical Package for the Social Sciences version 18.0 package (IBM Corp., Armonk, NY) was used for all statistical analyses. We carried out the statistical analyses in four stages, as follows.
Stage 1: Although many studies have reported that the three questionnaires are valid tools, it was necessary to confirm various factors including age, symptom duration, diagnosis type, and gender could influence the results of this study. For this, a multiple regression analysis of the mean scores for the K-VHI, K-VRQOL, and K-VCI was performed to verify whether age, symptom duration, type of diagnosis, and gender affected the results. Using the criteria outlined by Shoffel-Havakuk et al. [18], age and symptom duration were classified as follows: age above or below 60 years and symptom duration of more or less than 1 year, respectively.
Stage 2: To verify linear correlations between the K-VHI and its three subtypes (functional, physical, and emotional), the K-VRQOL, and the K-VCI, we used Pearson correlation coefficients.
Stage 3: We used the Mann-Whitney U test to compare the mean K-VHI scores with its three subtypes (functional, physical, and emotional), the K-VRQOL, and the K-VCI among the control and case group.
Stage 4: We used the receiver operating characteristics (ROC) curve to determine the sensitivity, specificity and the area under the curve (AUC) for each cut-off point and domain of the K-VHI, K-VRQOL, and K-VCI. The accuracy level of the AUC ranged from excellent to poor (0.9–1: excellent, 0.8–0.90: good, 0.7–0.8: fair, and 0.6–0.7: poor; a value of poor and 0.5–0.6: failure). P-values less than 0.05 were considered to be statistically significant.
RESULTS
The effects of age, symptom duration, type of diagnosis, and gender on questionnaire scores
A multiple regression analysis showed that the mean K-VHI, K-VRQOL, and K-VCI scores were not affected by age, symptom duration, diagnosis type, or gender in the case group (Table 2). The K-VHI scores were not significantly affected by age above 60 years (p=0.672), symptom duration longer than 1 year (p=0.515), diagnosis type (p=0.421), or gender (p=0.295); the K-VRQOL scores were not significantly affected by age above 60 years (p=0.377), symptom duration longer than 1 year (p=0.170), diagnosis type (p=0.385), or gender (p=0.742); and the K-VCI scores were not significantly affected by age above 60 years (p=0.431), symptom duration longer than 1 year (p=0.292), diagnosis type (p=0.116), or gender (p=0.330).
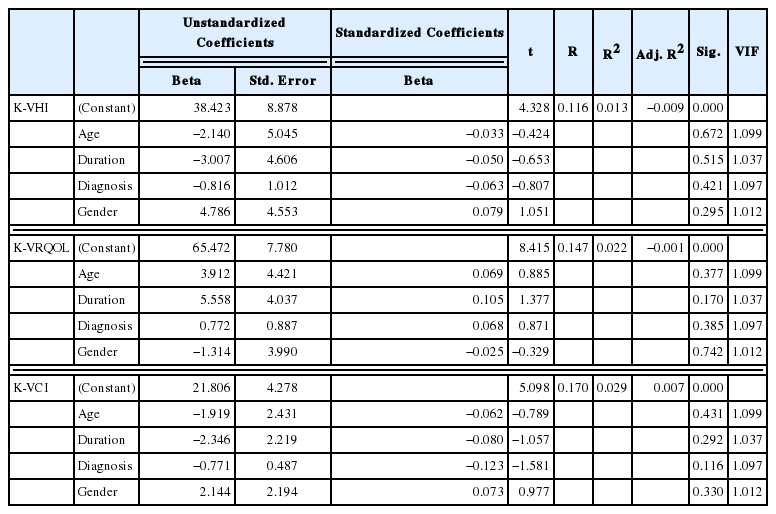
Multiple regression analysis for the effects of factors on the K-VHI, K-VRQOL, and K-VCI in case group
Correlations between the K-VHI, K-VRQOL, and K-VCI
Correlations between the K-VHI and its three subtype (functional, physical, and emotional), K-VRQOL, and K-VCI are presented in Table 3. All questionnaires used in the present study showed a significant correlation with each other (p<0.001).

Correlations between the K-VHI, three subtypes of K-VHI, K-VRQOL, and K-VCI
Descriptive statistics for the K-VHI, K-VRQOL, and K-VCI
To compare the mean scores of the K-VHI and its three subtype (functional, physical, and emotional), K-VRQOL, and K-VCI between the control and case groups, we used the Mann-Whitney U test (Table 4). The mean K-VHI and K-VCI scores for the case group with voice disorders were significantly higher than those of the control group (without voice disorders) (p<0.001). The mean K-VRQOL scores for the case group were significantly lower than those of the control group (p<0.001).
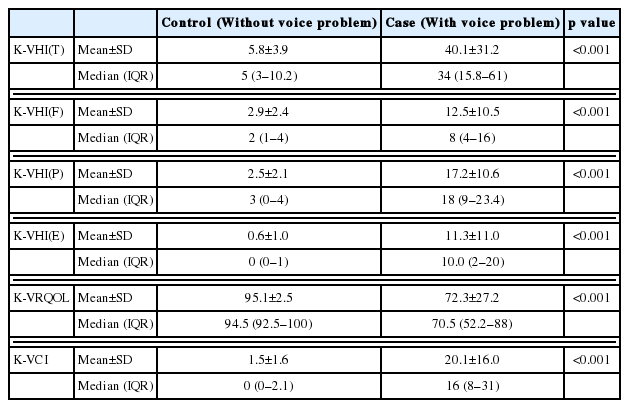
Descriptive statistics of K-VHI, three subtypes of K-VHI, K-VRQOL, and K-VCI in two groups
Cut-off points for the three questionnaires at which dysphonia was differentiated from normal voice
Based on the ROC curve test in our study; the cut-off points for K-VHI, K-VRQOL, and K-VCI that differentiate dysphonic voice from normal voice were 12.1, 91, and 6.1 points, respectively (Table 5). The AUC values for the three questionnaires were above 0.9, and the sensitivity and specificity for the three questionnaires were above 0.9.
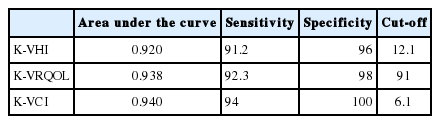
Sensitivity, specificity, and AUC of the K-VHI, K-VRQOL, and K-VCI cut-off points
DISCUSSION
In this study, we verified the diagnostic capabilities of these questionnaires for applicability in Koreans patients. The mean scores of the three questionnaires were not affected by age, symptom duration, diagnosis type, or gender and were in-line with previous studies [9,18,25]. This supports the generalized use of all three questionnaires in dysphonic patients and for a broad range of voice disorders.
There were significant correlations among the questionnaires used in present study. For the VHI and VRQOL, previous studies that the reported VHI was significantly correlated with the VRQOL (correlation coefficients range: −0.7–−0.9) [30–32]. For the K-VHI and K-VRQOL, significant correlation between two questionnaires was also reported (correlation coefficient range: −0.8–−0.9) [29,33]. For the VRQOL and VCI, there was a moderate correlation (correlation coefficients: −0.562) in a previous study [18]. And, for the K-VRQOL and K-VCI, significant correlation between the two questionnaires was reported (correlation coefficient: −0.897) [25]. Our study showed a higher correlation coefficient (−0.882) between the K-VRQOL and K-VCI, which is similar to previous research results on Koreans [25]. These results might suggest that the K-VRQOL and K-VCI are not significantly affected by cultural differences. We verified the significant correlation between the K-VHI and K-VCI in this study; these results were similar to previous research [25]. Catastrophization relates to aspects of the patient’s inner life (e.g., inner thoughts and beliefs) and is distinct from QOL and handicap which relates to aspects of the patient’s outer life. Our study supports many previous studies that have reported decreased functional health and well-being, as well as psychometrically-based physical and mental health in dysphonic patients [34–37].
The mean scores for all three questionnaires differed significantly between the case group and the control group in our study. Woisard et al. [38] showed that a VHI total score of dysphonia was 39.7 points, and that the ‘physical’ subtype was the highest score among the three subtypes. This was consistent with our K-VHI findings. Other researchers also noted the highest level of handicap in the ‘physical’ subscale [26,39]. The mean score for the K-VRQOL was 72.3 points in our case group, similar to studies by Aaby et al. (mean score: 74.5) [31] and Sielska-Badurek et al. (mean score: 75.5) [40]. The mean score for the K-VCI was 20.1 points in our case group, similar to the finding of Shoffel-Havakuk et al. (mean score: 22.5) [18] and Lee et al. (mean score: 21.6) [25]. These results might suggest that the three questionnaires were not significantly affected by cultural differences.
We found that at the cut-off points, all three questionnaires had relatively high sensitivities and specificities (above 0.9), and the AUCs (above 0.9) indicated excellent accuracy and high powers of discrimination. Our cut-off point for the K-VHI was equal to 12.1, similar to previous studies [26,27]. Previous studies reported a VHI cut-off point of 12 to be clinically relevant and useful for distinguishing patients with voice disorders from the controls group. Additionally, Ohlsson et al. [28] suggested that a VHI cut-off point of 13 be used to screen patients with voice problems. Thus, the VHI appears to have high validity and is relatively unaffected by cultural differences.
Our cut-off point for the K-VRQOL was equal to 91. Similarly, Behlau et al. [41] reported a cut-off point of 91.25 for the VRQOL to distinguish patients with voice disorders from the controls group. However, Morawska et al. [42] reported a cut-off point of 79 in a homogenous group of occupational voice users. The inter-study discrepancies in the VRQOL cut-off point may result from differing participant characteristics. Contrary to the present study and the study by Behlau et al. [41], the study by Morawska et al. [42] was conducted on a homogenous group of occupational voice users [42]. For this reason, the VRQOL scores of professional voice users with voice disorders may be lower than those of non-professional voice users with voice disorders; further these results may affect the cut-off point of the VRQOL [42].
Our cut-off point for the K-VCI was equal to 6.1. The K-VCI also had a relatively high sensitivity and specificity, and the AUC indicated excellent accuracy and a high power of discrimination. Although there were no previous reports on the VCI cut-off point that distinguishes the case group from the control group, the VCI is a valid tool for estimating the degree of catastrophization in patients with dysphonia [18,25]. Considering the results of previous studies and our study, it is important to also be deal with not only outer world factors such as QOL, but also the patient’s internal world (e.g., catastrophization) when screening and treating dysphonia. Inter-disciplinary team collaborations are necessary to implement improved screening, diagnosis, and therapy for patients with voice disorders. Through this process, we believe that the voice related problems of patients, which include everyday vocal tasks, external interactions, cognition, and the internal aspects of disability and interaction can be improved.
In this study, we analyzed the cut-off points for the K-VHI, K-VRQOL, and K-VCI for screening the dysphonic from normal voice and verified the diagnostic capability of the three questionnaires for Koreans. Thus, the results of this study can be used as criteria for screening for dysphonia. It is important to note that we only included Koreans in this study. In future studies, a large sample size will be necessary and multiple cultures will need to be included to evaluate the criteria needed to screen for dysphonia.
CONCLUSIONS
In this study, we provide evidence that the K-VHI, K-VRQOL, and K-VCI can be used to distinguish patients with voice disorders from the control group. Our results have excellent accuracy and a high power of discrimination and can be used to screen for dysphonia in Korean patients.
ACKNOWLEDGMENTS
The authors would like to thank all patients participated in this study.
Notes
STATEMENT OF ETHICS
The authors have no ethical conflicts to disclose.
DISCLOSURE STATEMENT
The authors have no conflicts of interest to declare.
FUNDING SOURCES
No funding was given.
AUTHOR CONTRIBUTIONS
All the authors fulfill the ICMJE Criteria for Authorship.
References
Appendices
APPENDIX A Korean-Voice Handicap Index (K-VHI)
현재 자신의 목소리 상태와 이 목소리가 삶에 어떠한 영향을 주는지에 대한 개인의 경험에 대한 사항입니다. 아래에 기술된 질문사항들을 읽고 해당하는 곳에 표시해 주십시오. (0= 전혀 없다 1= 거의 없다 2= 가끔씩 3= 거의 항상 4= 항상)
APPENDIX B Korean-Voice Related Quality of Life (K-VRQOL)
다음의 질문에 대해 본인이 느끼는 생각과 감정이 어느 정도인지 표시하십시오.
1= 문제가 전혀 없다 2= 약간 문제가 있다 3= 중간 정도 문제가 있다
4= 문제가 많다 5= 문제가 더 이상 나쁠 수 없을 만큼 심각하다