Development and usability of biofeedback system for water resistance therapy using sensor
Article information
Abstract
Purpose
The purpose of this study was to develop a water cup device for voice therapy as a biofeedback device for water resistance therapy (WRT), one of the semi-occluded vocal tract exercises (SOVTEs) using sensors. In addition, we explore the usefulness of the system for training in voice therapy by implementing water resistance phonation through newly developed devices.
Methods
Using Arduino, the water resistance value was measured using a water level sensor, and a system was developed to visually implement the water resistance value and duration of exhalation and vocalization according to the change in water level caused by bubbles. Visual feedback was provided using LED sensors that represent colors according to the height of the water level. The WRT step was performed on six normal adults (male 3 and female 3) to implement changes in water level change amplification rate according to tube diameter and depth, and quantitatively analyzed.
Results
The experiment showed that different LED colors were displayed depending on the resistance value of the water level. The LED’s brightness decreased as the width of the silicone tube diameter became larger in the bubble according to the tube diameter. Moreover, compared to 5 mm or 7 mm, a tube diameter of 10 mm showed the lowest amplification rate, regardless of with or without phonation. A depth of 2 cm, with the tube tip submerged in water, demonstrated the lowest amplification rate with or without phonation, compared to 4, 7, and 10 cm.
Conclusions
The newly developed cup device for water resistance therapy was easy to give visual feedback according to changes in water level and helped to identify objectively by quantifying the performance of the target. This system may help clinicians and patients not only in clinical situations but also in practice at home during voice training.
INTRODUCTION
Voice disorders can occur throughout life, especially in the United States, with more than 5 million children reported to occur, and in Korea, preschool-aged children showed 34.9% of auditory-perceptual evaluation and 22.2% of acoustic evaluations [1,2]. Also, in older adults, the incidence of voice problems is estimated between 12 and 35% [3]. In addition, it has been reported that there are more voice disorders in professional voice users than in the general population [4].
To treat voice disorders, voice treatment is performed with behavioral therapy along with surgery or medication. Voice therapy includes indirect voice therapy to reduce factors contributing to vocal injury, such as voice rest and vocal hygiene, and direct voice therapy to teach or change voice production methods [5].
Among them, physiological voice therapy programs aim to improve balance among the main subsystems involved in voice production, that is, respiration, phonation, and resonance and to improve strength of laryngeal muscles, and to develop healthy vocal fold vibration[6–7]. In physiological voice therapy, semi-occlued vocal tract exercise (SOVTE) is a method of vocalization by closing the front or back of the vocal tract and is used to control the shape of the vocal tract to affect the sound source [8].
Vocal Function Exercises (VFE) [9], Accent Method of Voice Therapy (AM) [10], and Resonant Voice Therapy (RVT) [11] have long been used as holistic or integrated approaches focused on reconstructing the overall physiology of voice production.
In addition, lip or tongue trill has already historically been used as a method of SOVTE for a long time as a vocal warm-up for singers and voice professionals, and recently SOVTEs, such as tubes or straw phonation, are widely used [8].
More recently, one of the Semi-Occluded Vocal Tract Exercises (SOVTEs) is a tube or straw phonation that is widely used with other tubes, either freely in the air or in water, such as LaxVox [8,12–14]. Among them, the water resistance tube phonation method is to increase oral pressure so that phonation can occur while bubbling [15,16]. At this point, the bubble that occurs allows us to know how long airflow, or breathing, is supported.
WRT is available for both hyperfunctional and hypofunctional dysphonia patients, with varying water resistance depending on the depth of the tube from the water surface and tube diameter, and its effect on vocal tract [12].
In tube phonation, the process of the water resistance therapy (WRT) is as follows. First, breathing and relaxation training are performed. Second, breathing deeply through the nose and exhaling through the mouth is done to make long bubbles without phonation. Third, /u/phonation is made while the bubble strength remains constant from the beginning to the end of vocalization.
In the fourth step, sustained phonation and staccato training are conducted at a comfortable pitch, at a low pitch, and at a high pitch. Fifth, gliding is conducted from low to high pitch, or from high to low pitch.
Finally, in the sixth step, generalization training, the silicone tube is put into the water and bubbles up to maintain /u/ phonation. During vocalization, the subject maintains the optimal /u/ phonation while removing the tube from the mouth.
In addition, /u/ phonation is performed without a silicon tube while varying the pitch and intensity. At this time, generalization training is conducted in the order of syllable-word-sentence [17,18].
On the other hand, direct voice therapy requires modification of vocal function, and respiratory, musculoskeletal, as well as auditory and somaticsensory modification [19]. At this point, biofeedback is very useful as a monitoring tool, for example, when it is difficult for a patient to pay attention to their sensation of vibration/motor (e.g., discrimination), visual processing, or auditory discrimination.
Previous studies have demonstrated that biofeedback has been effective in improving voice function, reducing laryngeal tension and helping improve voice quality, thereby significantly eliminating voice problems [20].
To date, voice therapy methods are mostly modeled by speech-language pathologists who teach patients to imitate them, which makes it difficult to provide adequate feedback or determine how well they perform.
The bubbles may play an important role, providing visual, auditory, and tactile feedback for both the clinician and patient during the exercise. However, during the WRT, patients need to maintain constant breathing pressure or vocalization, which is critical to properly monitor their performance and provide appropriate feedback to the patients.
Therefore, SOVTE is the most commonly used voice therapy technique in clinical practice, but it is very difficult to determine whether both the speech-language pathologist and patient understand or perform the tasks of each step of these voice therapy techniques correctly. To overcome these shortcomings, biofeedback among the direct voice therapy methods provides information on the physiological aspects of voice behavior seen by the patient, through auditory, visual, tactile, and kinematic pathways [21]. In addition, intervention delivery methods of voice therapy include external approaches such as steps, modeling, psychological support, and teaching, as well as internal approaches such as the patient’s own self-evaluation and self-modification, and self-correction. These are programs that permit feedback, and accurate practice at home.
Thus, if a system is developed that can provide feedback and quantify the patient’s performance, it could provide efficient monitoring and self-training of voice therapy for both clinicians and patients.
In this study, we developed a water cup device for voice therapy using sensors as a biofeedback device for water resistance voice training.
Furthermore, the authors would like to examine the usefulness of the system for training in voice therapy by implementing water resistance phonation according to tube diameter and tube depth from the water surface.
METHODS
Development of biofeedback water cup system
In order to quantitatively measure the height change of water bubbles, the water resistance value was measured using an arduino in a cup containing water, and a system was developed to visually implement the water resistance value and duration of exhalation and phonation time according to the water level height. It was also designed to provide visual feedback using LED sensors that represent colors according to water level height (Figure 1).

Biofeedback water cup system for water resistance therapy.
The water level sensor was connected to the Arduino and the code was applied to verify the operation of the water level sensor.
During bubbling, the lid was manufactured by modeling it with a 3D printer to prevent water from splashing out and to secure the water level sensor and silicone tube. The manufactured lid is shown in Figure 2.
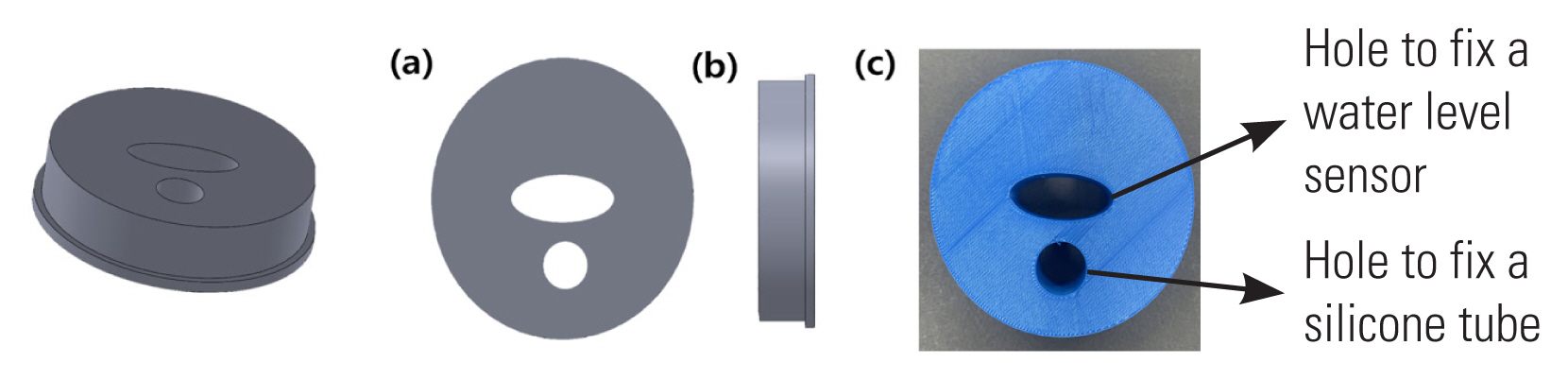
(a) top side (b) right side of the manufactured lid, (c) the actual model.
In this study, the size of the cup used was 75×223 mm.
The resistance value was confirmed by filling the water cup with 100 mL of water to see how the output resistance changes with the change in water level using a water level sensor in the newly developed 1 L water cup device.
The water level sensor depends on the water level, representing the output with variable resistance values. The higher the water level, the lower the resistance value, and the lower the water level, the higher the resistance value.
According to the measurement result of the water level in an 1 L water cup, the higher the water level, the lower the resistance value.
In addition, experiments showed that the resistance value changed from 4 cm above the height of the water level sensor, and that the resistance value changed above 300 mL of water (Figure 3).
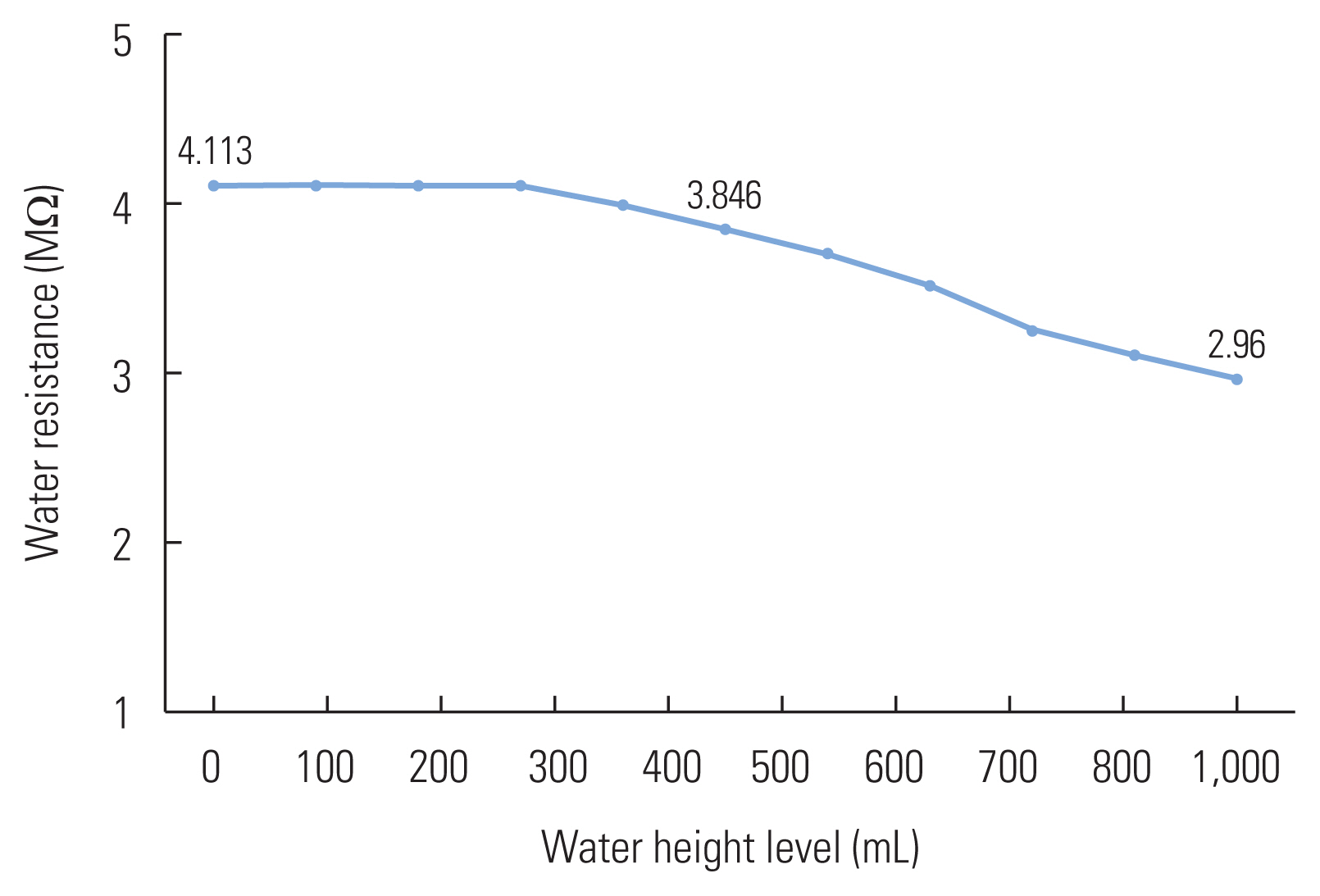
Resistance output according to water level.
Participants
This study was approved by the Research Ethics Committee of the Institutional Review Board (IRB), Daegu Catholic University. Participants were 6 normal young adults, 3 men and 3 women, aged 23 to 29 years (mean age 26.8±2.4), who agreed to participate in the study in advance and signed an Informed Consent Form.
The following exclusion criteria were adopted: voice complaint; history of diagnosis of laryngeal lesions and/or vocal disorder (past or present); infection of the upper airways at the time of data collection; history of any health problems/changes (past or present) that could negatively influence phonation; experience in vocal training or voice therapy (past or present).
Experiment procedure
Experiment 1: Performance of water cup system for water resistance therapy
In a 600 mL cup of water, the participant sat in a chair and immersed the tube in the water through a silicone tube, breathing for 5 seconds to form a bubble.
Using the water level sensor and the light bulb, it was measured at 5 seconds before, during, and after breathing, and stored on a PC.
Using this, the range of output values in the arduino code was designated and visible changes in LEDs were confirmed depending on the bubble level.
The results were compared when bubbles were generated without vocalization according to the changes in the diameter of the silicone tube (5, 7, and 10 mm).
Experiment 2: Change in water level according to tube diameter and tube depth
First, the participant was comfortably relaxed in the chair. Each step of the WRT was carried out using a newly made voice therapy water cup device. The end of the silicone tube was submerged in water while participants conducted exercises to understand each step and conducted the experiment. Each phase of the WRT is as follows.
a. Bubbling without phonation, b. Bubbling with sustained vowel /u/ phonation at a comfortable pitch, c. Bubbling with gliding from the lowest to highest pitch, d. Bubbling with gliding from the highest to lowest pitch, e. Bubbling with singing “happy birthday” through the tube.
At this time, silicone tubes were the same length of 35 cm, and the variations in the diameter of the tubes (5, 7, 10 mm) and the depth of the tubes (2, 4, 7, 10 cm) from the surface of the water were visually implemented.
Furthermore, the results of the amplification rate were compared by quantitatively measuring the change in water level during /u/ vowel phonation, depending on the changes in silicone tube diameter (5, 7, 10 mm) and the depth of the tube (2, 4, 7, 10 cm) from the surface of the water using a 35 cm in length.
RESULTS
Color change of LED according to bubble level
In this study, a developed voice therapy water cup device was used to instruct the subject to maintain a bubble of more than 4 cm from the original height of the water level and to give real-time feedback on how high the bubble can be blown using LED sensors.
Different LED colors were displayed depending on the resistance value of the water level (Figure 4, Table 1).
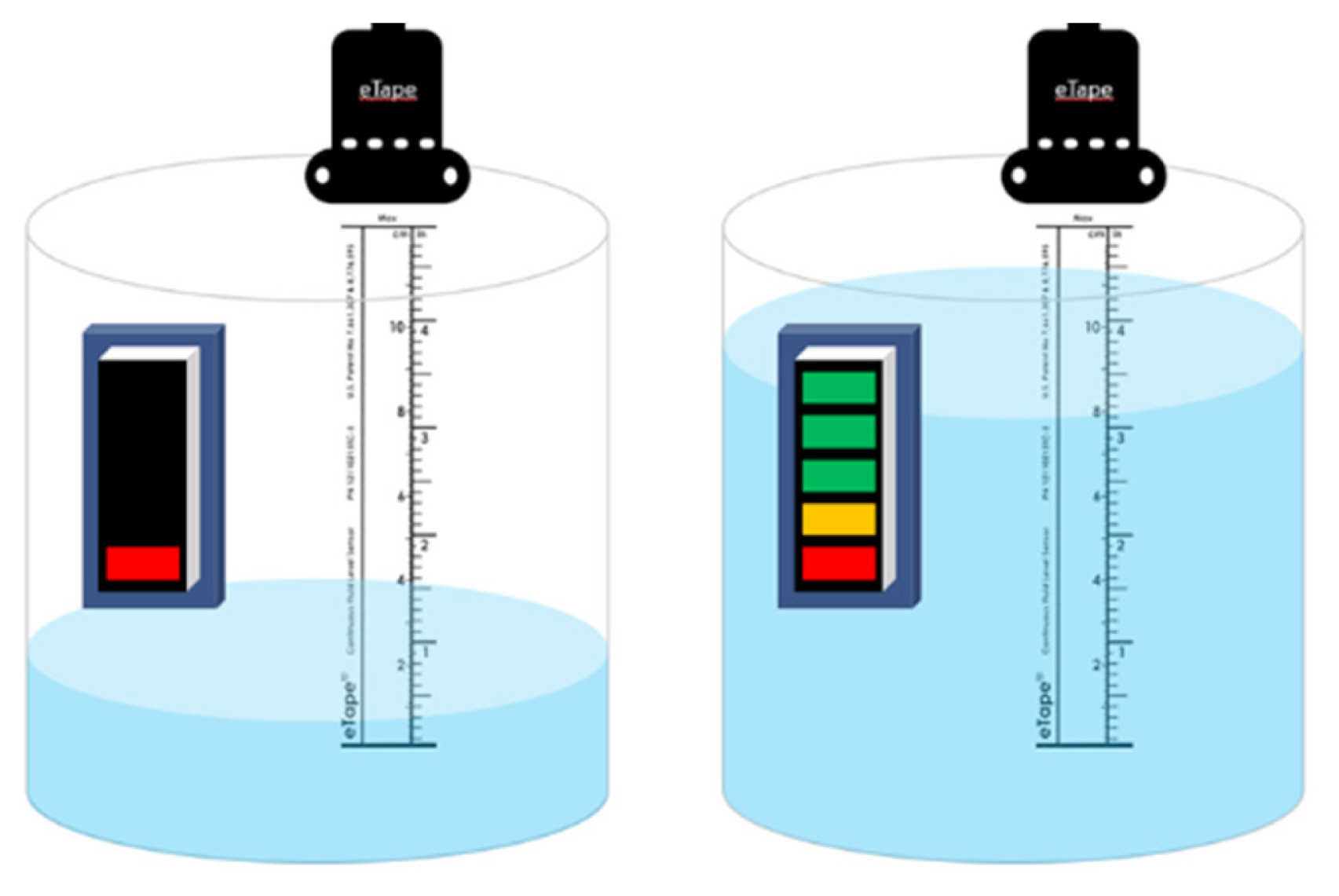
LED color changes with predicted water levels.

LED changes according to actual water level measurements
LED changes according to tube diameter
The LED’s brightness decreased as the width of the silicone tube diameter became larger in the bubble according to the tube diameter. Therefore, experiments have shown that the larger the tube diameter, the lower the height of the water changes (Figure 5).

LED changes according to tube diameter.
Water level height according to tube diameter
As a result of measuring the power of the sensor at bubble ime according to the tube diameter, the amplification rate of the power value increased as the diameter of the silicone tube increased.
Figure 6 shows an example display of the the amplification rate of the power value at each different tube diameter. In particular, in the case of tubes with a diameter of 10 mm, it was possible to observe that breathing ability decreased over time, resulting in a faster return of the output to its original state.
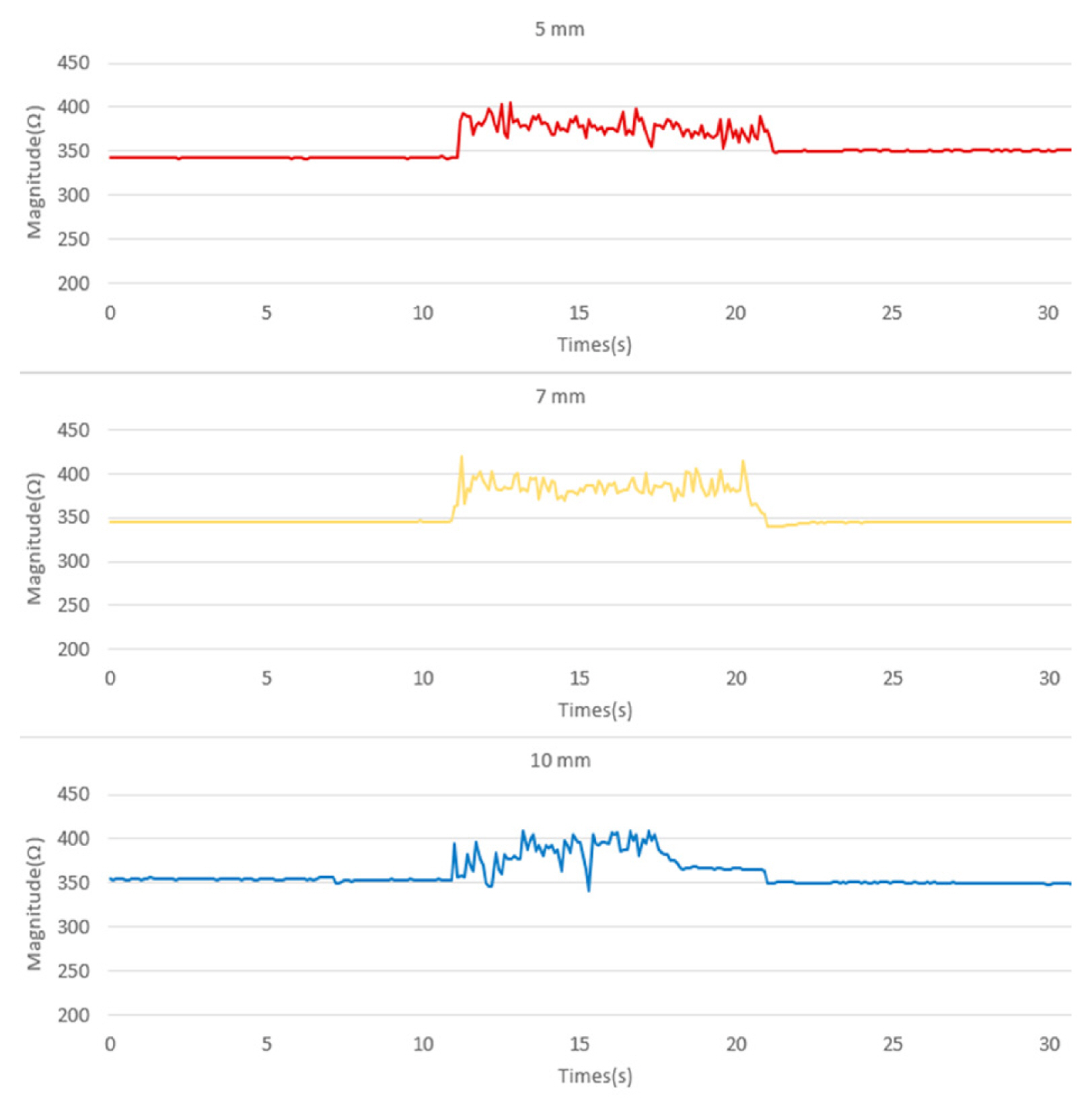
Real-time water level output changes during bubbling according to tube diameter.
Water level change by WRT stage depending on tube width and depth of water depth
Figure 7 shows the results of visual implementation of the water level change by WRT step according to the tube diameter (5, 7, 10 mm). In addition, the results of visual implementation of the water level change by WRT phase according to tube depth (2, 4, 7, 10 cm) are shown in Figure 8.
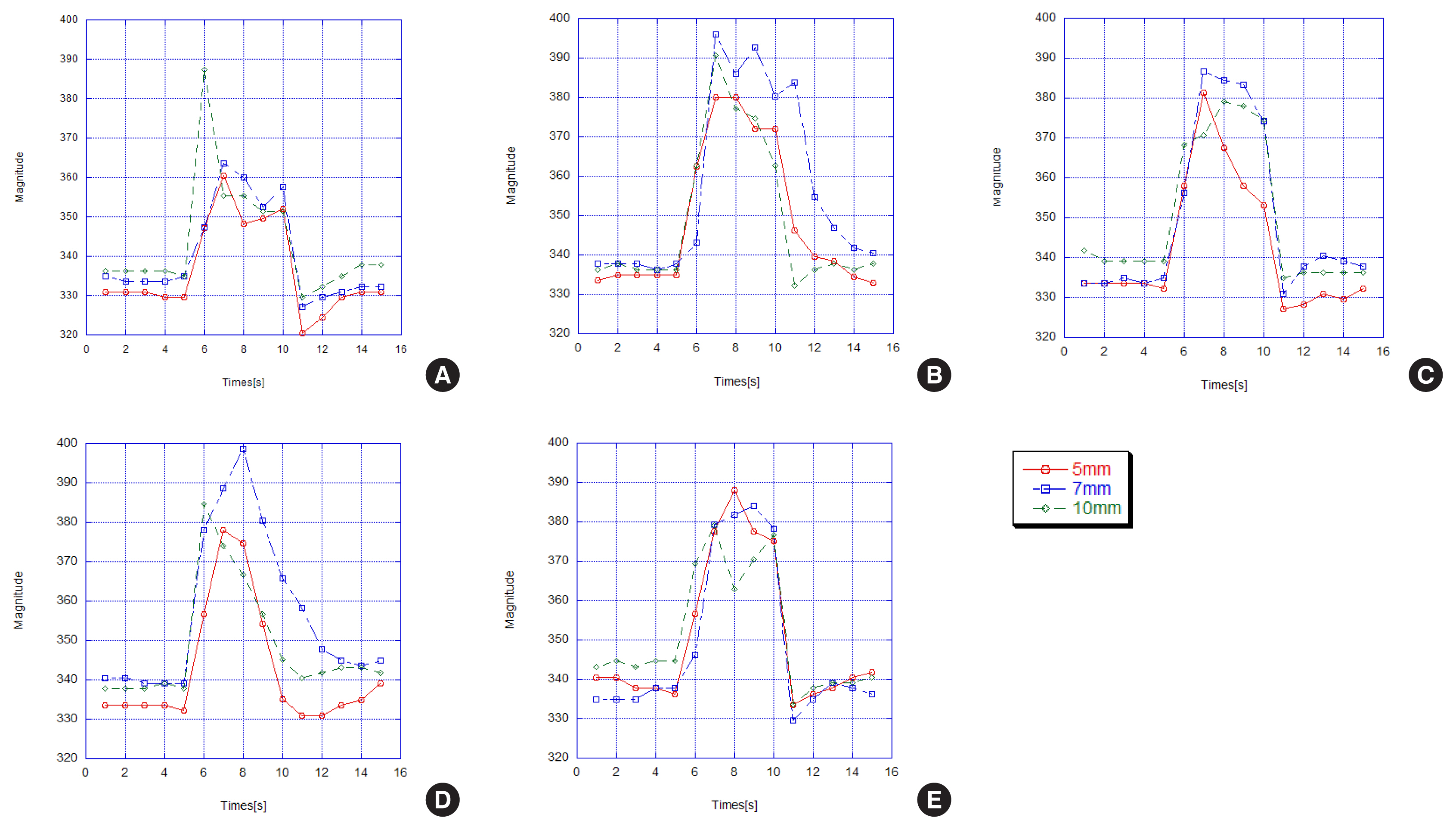
The fluctuation in water level at each stage of the WRT at a depth of 4 cm with different tube diameters (5, 7, 10 mm) for a female participant; (A) bubble without phonation, (B) bubble with phonation, (C) gliding from low to high pitch phonation with bubble, (D) gliding from high to low pitch phonation with bubble, (E) singing ‘happy birthday’ with bubble.

The fluctuation in water level at each stage of the WRT using a 5 mm tube diameter at different water depths (2, 4, 7, 10 cm) for a female participant; (A) bubble without phonation, (B) bubble with phonation, (C) gliding from low to high pitch phonation with bubble, (D) gliding from high to low pitch phonation with bubble, (E) singing ‘happy birthday’ with bubble.
Comparison of water level change amplification rate between bubbles with and without phonation
The amplification rate of water level change according to tube diameter in the bubbling without phonation and with sustained vowel /u/ phonation is shown in Figure 9. Compared to 5 mm or 7 mm, a tube diameter of 10 mm showed the lowest amplification rate, with or without vocalization.

Comparison of amplification rate of water level change between bubbling with and without phonation according to tube diameter.
In addition, the amplification rate of water level change according to tube depth during bubbling with and without /u/ phonation is shown in Figure 10. The depth of 2cm from the surface of the water showed the lowest amplification rate, regardless of whether or not it was vocalized, compared to 4, 7, and 10 cm.
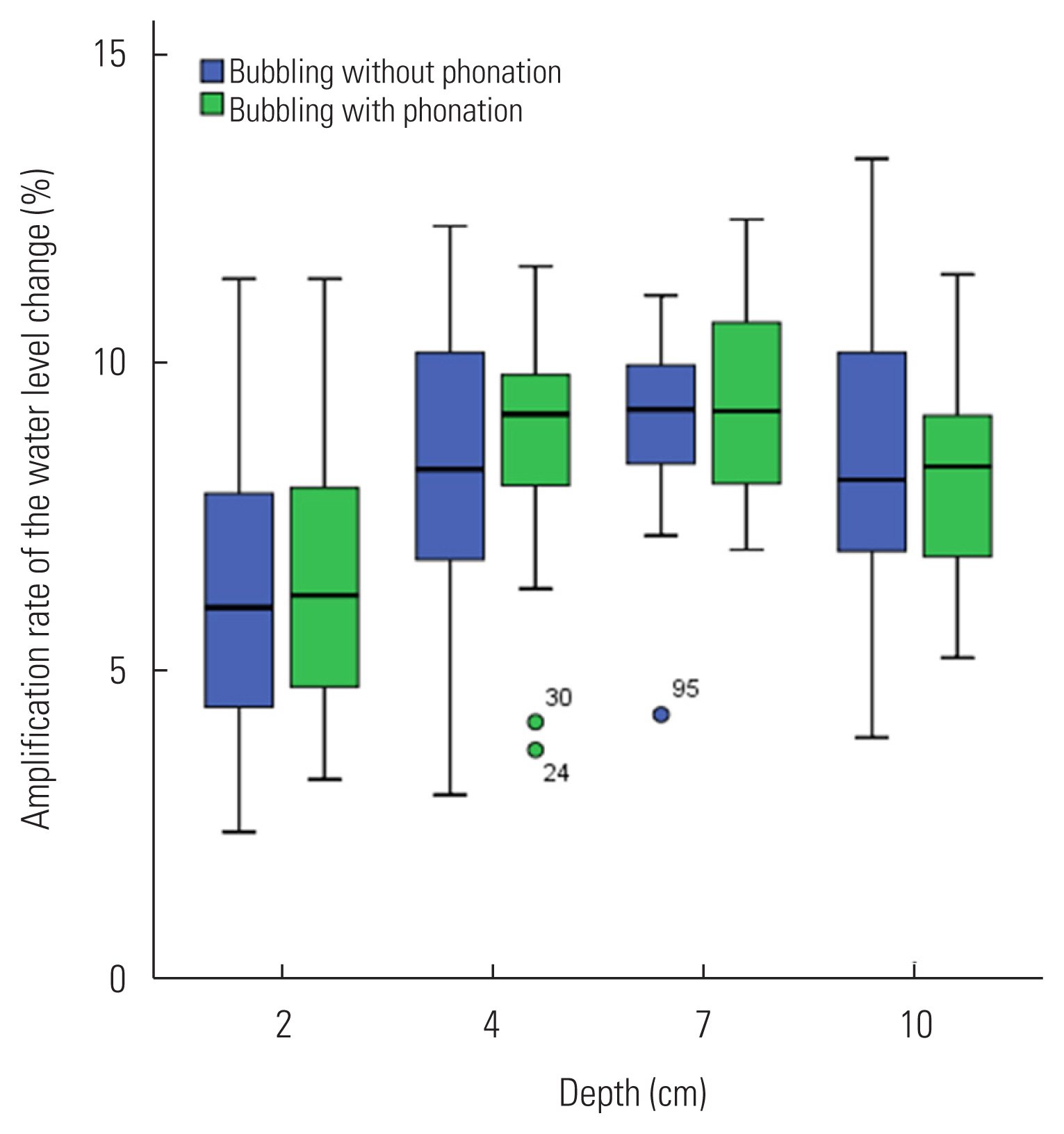
Comparison of amplification rate of the water level change between bubbling with and without phonation according to tube depth from the water surface.
DISCUSSION AND CONCLUSIONS
This study developed a water resistance phonation system for voice therapy composed of water level sensors, LED, and arduino to measure the height of bubbles. Using a water level sensor, the height of the bubble was objectively quantified during water resistance phonation, and visual feedback was provided.
As a result of this study, red, yellow, and green LEDs were illuminated depending on the water level, making it easier to give visual feedback according to the bubble level. Thus, the patient will be able to set a water level target and practice it step by step.
Meanwhile, various tubes such as plastic, glass, and silicone are used for semi-occluded vocal tract exercises. The LaxVox® tube was developed by a Finnish company and it proposes to combine SOVTE with water resistance [16].
In current study, flexible silicone tubes that bend well to ensure that the target maintains the optimal posture were used when blowing.
Once the resonance and silicone tubes were submerged, the back pressure had to overcome the pressure equivalent to the depth of the water before the flow could occur.
When the tube end is submerged into water during continuous phonation, the bubbles cause oscillation in the oral pressure. WRT is available for both patients with hyperfunctional and hypofunctional voice disorders, and it has been reported that water resistance varies depending on the depth of the tube and its effect on vocal tract and vocal fold vibrations [12].
Moreover, when a tube is submerged in water, extra resistance is added due to hydrostatic pressure, which is dependent on the depth of immersion.
A study by Andrade et al. [22] reported that changes in tube diameter and depth have a greater impact on the back pressure than the length of the tube.
The developer of the WRT method, Antti Sovijärvi, recommended tubes between 26 and 28 cm in length with a diameter of 9 mm for adults while tubes for children should be between 24 and 26 cm in length with a diameter of 8 mm [23]. However, there is no evidence for why these specific tube lengths and diameters would be more appropriate than others. Several studies used various tube widths and depths for SOVTE.
Simburg and Lane [12] proposed three versions of the resonance tube in water according to training purposes. For example, in order to treat hyperfunctional voice disorder or vocal nodules, Simburg and Lane recommended continuous phonation with tube ends submerged in 1 to 2 cm of water. Short phonation is recommended when treating patients with insufficient vocal fold closure, allowing the tip of the tube to be submerged at a depth of 15 cm, similar to the pushing method. Similar voice training methods use continuous phonation through silicone tubes immersed in water using the LaxVox technique. The recommended depth of water for this technique is 1 to 7 cm, which is deeper than the resonant tube phonation.
In the current study, experiments with normal young adults showed that the height of the water level depends on the diameter of the tube when the tube is applied differently to the length of the same tube, which affected the resistance value of the water. In other words, the wider the diameter of the tube, the more difficult it was for subjects to blow and maintain breathing. This phenomenon is expected to be due to the lower back pressure due to the lower flow resistance of the wide tube, which is less than that of the 5 mm or 7 mm tube.
In addition, Andrade et al. [22] reported that submerged resonance and silicone tubes produced almost constant Pback depending on the depth of the water compared to thinner straws in air.
In addition, the depth of water has also been reported to affect the oral pressure amplitude of oscillation during bubbling. The largest value of the vocal fold oscillation amplitude occurred at a depth of 3–7 cm, indicating that the vocal fold oscillation does not change at depths greater than 3 cm. Wistbacka et al. [23] suggested that submersion of the end of the tube deeper than 3 cm would not significantly increase the amplitude of the oral pressure oscillation.
Similarly, Guzman et al. [24] found that there was no significant difference in the peak-to-peak amplitude of the oral pressure modulations during bubbles at 3 cm and 10 cm water depths using a 55 cm silicone tube for 45 participants.
In our study, three 35 cm-long silicone tubes with different diameters (5, 7, and 10 mm) were immersed at four different water depths (2, 4, 7, and 10 cm), and the amplification rate of the water level change ranged from 2.46 to 13.29%.
In particular, in this study, the water level change amplification rate declined in a tube with a diameter of 10 mm, and the water depth was the smallest at 2 cm. In addition, as with previous studies, there was no difference in water level changes at 4 cm and 10 cm water depth.
It is believed that the wider the tube diameter, and the more shallow the water depth, and the lower the water resistance, which resulted in a lower back pressure, and a lower amplification rate of the water level change.
Meanwhile, a study by Granqvist et al., [15] conducted a resonance tube phonation on two people and analyzed vocal fold vibrations, and found that the deeper the tube is immersed (from 2 cm to 6 cm), the higher the open quotient. This seems to have increased vocal abduction due to increased back pressure.
In our study, only a few normal adults were investigated for changes in water level according to tube diameter and depth. Future studies will be able to help build clinical guidelines by looking at scientific evidence of tube diameter or depth depending on the type of functional voice disorders (hypo-or hyperfunctional) using the device we have developed.
Nevertheless, in this study, a newly developed voice therapy water cup device using sensors identified several mechanisms available to clinicians to provide appropriate visual goal for patients. These goals could help improve the reproducibility of exercises during training at home as well as in clinical practice.
ACKNOWLEDGMENTS
The research has been supported by tthe Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2020S1A5A2a0145868).
No conflicts of interest were reported by the authors.