INTRODUCTION
Dysphagia is a disorder that disrupts the efficiency of swallowing and can lead to serious consequences of patient safety and quality of life. Over 50% of head and neck cancer survivors suffer from dysphagia, and approximately 30–50% stroke survivors suffer from pharyngeal dysphagia [1,2]. Head and neck cancer has classically been treated using three different methods: surgical excision, radiation, and chemotherapy, which are either implemented alone or in combination with others. Any one of these remediation approaches can increase the likelihood of patient dysphagia. Chemotherapy and radiation keep structures intact, but these structures may not function at highest potential for swallowing post-treatment (e.g., fibrosis) [3–5]. Dysphagia is common following a stroke and the length of the disorder varies depending on lesion, location and severity of the infarction. Aspiration occurs at a high rate in stroke survivors, mostly due to sensation deficits in the pharyngeal and laryngeal zones. The negative consequences that individuals with dysphagia experience can include dehydration, malnutrition, aspiration pneumonia, and, most severely, death [6,7].
Swallowing is divided into three physiologic stages: oral, pharyngeal, and esophageal [8]. For safe and efficient swallowing, laryngeal closure must be adequate to limit the risk of aspiration. During the pharyngeal stage, the epiglottis should flip inferiorly, while the arytenoid cartilages move in a superior-anterior motion. When these structures meet, the airway will close to prevent any food or liquid from entering the laryngeal vestibule, trachea, or lungs [9]. Once the airway has been shut, depending on how much bolus is being swallowed, the closure duration must be long enough to prevent any aspiration during or post-swallow [10,11]. Typically, the initiation of laryngeal closure should occur once the bolus passes the ramus of the mandible. To accurately calculate initiation of laryngeal closure whilst analyzing videofluoroscopic swallowing examinations (VFSEs), one measures the difference in time between the bolus passing the ramus of the mandible and the first contact of the epiglottis and arytenoid cartilages. When calculating the duration of laryngeal closure, one must note when the epiglottis and arytenoids first meet, and when they separate.
The purpose of this study was to examine the difference of two laryngeal closure measures during swallowing among stroke survivors, head and neck cancer survivors, and healthy controls. Temporal measurements of the oral and pharyngeal stages have been shown to be reliable tools for distinguishing normal and abnormal swallowing physiology [12–14]. In this investigation, initiation of laryngeal closure (ILC) and laryngeal closure duration (LCD) were analyzed. The outcomes of this study seek to provide clinically relevant information for differential diagnosis of these two disordered populations with swallowing disorders.
METHODS
Subjects
There were a total of 45 individuals’ VFSEs in this study: 15 head and neck cancer survivors, 15 stroke survivors, and 15 healthy normal controls. All VFSEs came from the Ohio University Swallow Laboratory database. Participants were age-matched across the three groups, the mean ages and standard deviations were as follows: head and neck cancer survivors (M=53 years), stroke survivors (M=56.53 years), and healthy controls (M=54.47 years). Specific inclusion criteria as follows: 1) all individuals in this study had no prior presence of a swallowing disorder, and 2) head and neck cancer survivors were post-treatment for their cancer.
Head and neck cancer survivors had varying cancerous lesions of the oral cavity (n=6), nasopharynx (n=2), pharynx (n=3), and larynx (n=4). Specific lesions of oral cancer included tongue base cancer (n=5) and tonsil cancer (n=1). Examples of pharyngeal lesions included supracricoid laryngeal cancer (n=2) and glottic cancer (n=1). Stroke survivors presented with lesions in the following areas: cortical (n=8), subcortical (n=4), and cerebellum (n=3). Specific cortical lesions include the frontal lobe and the temporal lobe. Subcortical lesions include the corona radiata and the thalamus. The healthy controls in this study were recruited on a volunteer basis. Internal review board (IRB) approval was granted for this investigation.
Videofluoroscopic Swallowing Examination Procedure
The VFSEs of head and neck cancer survivors, stroke survivors and healthy controls were retrieved from the VFSE database in the Ohio University Swallowing Research Laboratory. The VFSE procedure was performed as follows: The patient or volunteer was seated upright in either a stretcher chair or wheelchair for the examination. The VFSE was collected using a mobile C-arm X-ray and recorded with a 100 ms digital video timer (TEL Video Products Model VC 436). The fluoroscopic tube was focused in the lateral plane on the oral cavity and the nasopharynx to below the upper esophageal sphincter (UES) area. For this investigation, each participant swallowed two 5ml boluses of thin liquid consistency. The thin liquid was a mixture of water and barium (E-Z-HD barium sulphate powder).
Procedures for Temporal Measurements of Laryngeal Closure
This study focused on two airway protection mechanisms of oropharyngeal swallowing: ILC and LCD. ILC was measured as the time (s) between the bolus head passing the ramus of the mandible and the first contact of the arytenoids and epiglottis. LCD was measured as the time (s) between the first contact of the arytenoids and epiglottis and the final contact of the arytenoids and epiglottis. From the images of Figure 1, ILC was calculated by subtracting Image A (bolus passing ramus of mandible) from Image B (first contact of arytenoids and epiglottis) across all participants. LCD was calculated by subtracting Image B (first contact of arytenoids and epiglottis) from Image C (final contact of arytenoids and epiglottis). To accurately analyze the sequential transition timings, the researchers used a slow-motion, frame-by-frame analysis using a 100 ms video timer on the software Adobe Premiere Pro CS5.5. A certain level of clarity was required when determining whether a VFSE could be included in the analysis. To accurately determine the specific timings, structures such as the epiglottis and arytenoid cartilages needed to be visible. In total, 90 swallows were submitted for transition times and 86 swallows were analyzed. Four swallows were missing from 3 head and neck cancer survivors due to poor visibility of laryngeal closure.
RESULTS
Reliability
The first judge reanalyzed nine subject’s swallows for a second time for intra-rater reliability measures. Intra-rater reliability was measured using the intraclass correlation coefficient (ICC). Intra-rater reliability was as follows: ILC (ICC=0.99, p<0.01) and LCD (ICC=0.99, p<0.01). A second judge analyzed nine subject’s swallows. Inter-rater reliability was as follows: ILC (ICC=0.96, p<0.01) and LCD (ICC=0.99, p<0.01).
Initiation of Laryngeal Closure
The means (M) and 95% confidence intervals (CIs) of the ILC across the three groups are shown in Figure 2. There was a significant difference across all groups for ILC (F(2, 84)=3.62, p=0.03). A post-hoc Tukey analysis showed that there was a significant difference between the stroke survivors (M=0.68 seconds) and normal controls (M=0.10 seconds) at p=0.025; however, there was no significant difference between stroke survivors and head and neck cancer survivors (M=0.30 seconds) nor between head and neck cancer survivors and normal controls. Stroke survivors showed the longest delay of initiation of laryngeal closure, and head and neck cancer survivors the second.
Laryngeal Closure Duration
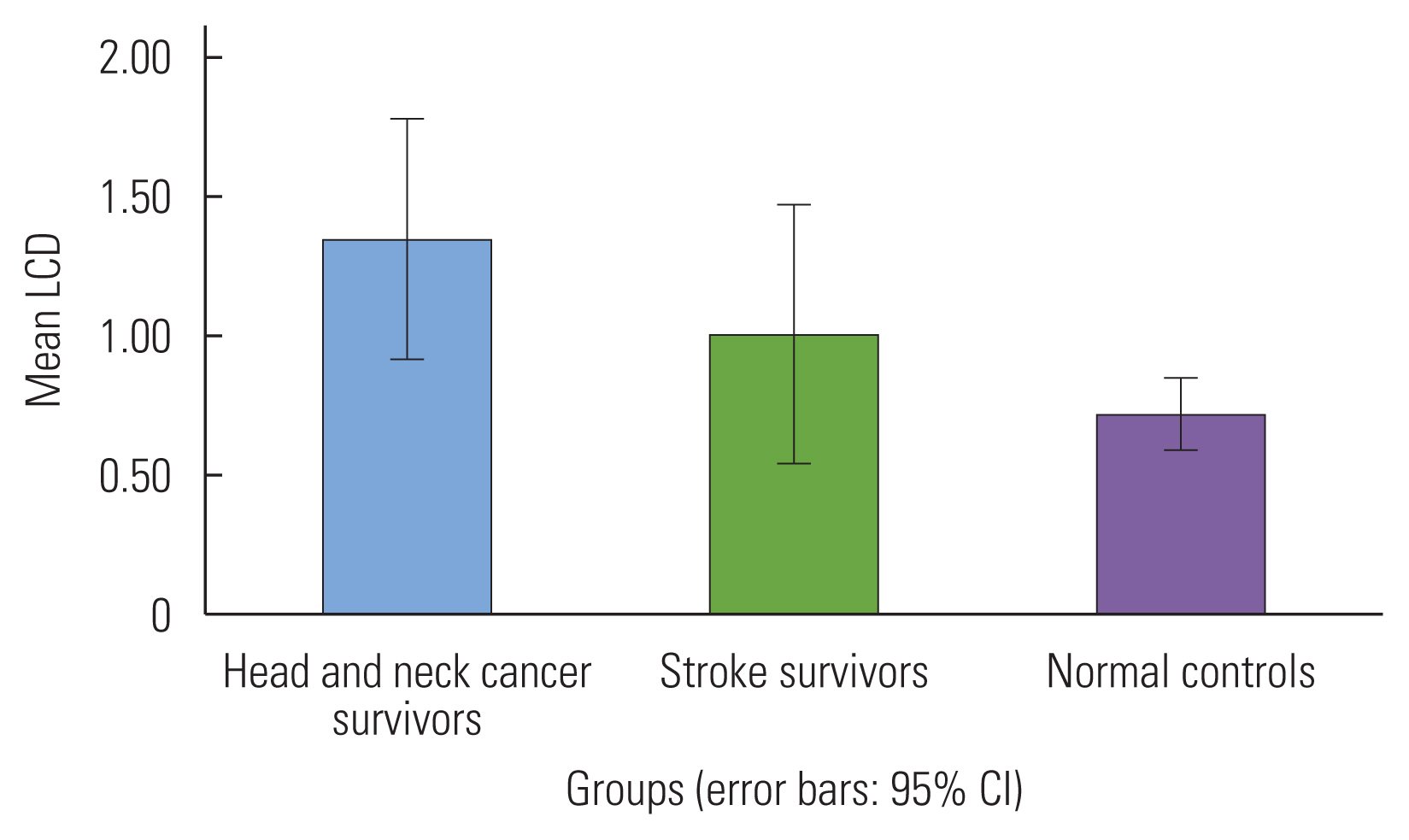
The means (M) and 95% CIs of the LCD across all three groups are shown in Figure 3. There was no significant across all groups for LCD (F( 2, 84)=2.99, p=0.06). A post-hoc Tukey analysis showed that there was a significant difference between the head and neck cancer survivors (M=1.34 seconds) and normal controls (M=0.72 seconds) at p<0.01; however, there was no significant difference between stroke survivors (M=1.00 seconds) and head and neck cancer survivors nor between stroke survivors and normal controls. Head and neck cancer survivors showed the longest laryngeal closure duration, and stroke survivors the second.
DISCUSSION
The purpose of this study was to determine differences across two airway protection mechanisms: ILC and LCD among head and neck cancer survivors, stroke survivors, and age-matched healthy controls. Results provided evidence for significantly longer ILC in stroke survivors compared to controls; however, head and neck cancer survivors’ ILC was not significant compared to the other groups. For ILC, stroke survivors tended to have the longest duration for airway closure initiation, followed by head and neck cancer survivors, and finally, the healthy controls exhibited the shortest duration for ILC. For LCD, head and neck cancer survivors exhibited a significantly longer average duration compared to normal controls; however, the stroke survivors did not differ significantly from the other groups. With respects to group differences, head and neck cancer survivors exhibited the longest duration, followed by the healthy controls, and stroke survivors exhibited the shortest amount of time for LCD. These results indicate that stroke survivors tend to have difficulty initiating the pharyngeal swallow and head and neck cancer survivors tend to maintain the duration of airway closure during the swallowing.
Adequate airway closure is pivotal for safe and efficient swallowing [15]. The results provided information that stroke survivors had significantly delayed initiation of laryngeal closure compared to the healthy subjects. The head and neck cancer survivors also took longer to initiate laryngeal closure; however, it was not significantly delayed compared to the healthy subjects. As noted in a prior study, typical ILC is approximately 0.20 seconds for healthy subjects [11]. In our study, we found that ILC for healthy subjects was approximately 0.10 seconds. Both the stroke survivors and head and neck cancer survivors exhibited longer ILC (0.68 and 0.3 seconds) than normal controls. Increased ILC raises concern that delayed pharyngeal swallow initiation is related to delayed pharyngeal swallow response, and the risk for aspiration increases in these populations [11].
It is noted in previous studies that there is evidence for longer pharyngeal delay in stroke survivors [16,17]. The longer pharyngeal delay in stroke survivors compared to head and neck survivors and healthy controls contributes to delayed and inadequate movement of the tongue and pharyngeal muscles, which are supposed to work in synchrony for safe swallowing. When these muscles do not work in a synchronous manner, the epiglottis and arytenoid cartilages are not alerted in time to close the airway by the central pattern generator swallowing center. This leads to a decrease in efficient and timely airway closure.
The head and neck cancer survivors differed from the stroke survivors with ILC, although, not significantly. There does appear to be a deficit with timeliness of laryngeal closure in this population. Four head and neck cancer survivors who had either radiation, chemotherapy, or surgical excision in the areas of the larynx showed longer delay of laryngeal closure than other patients in this group. Previous research states that individuals who have undergone surgical removal or radiation of the larynx can have difficulties with airway protection [3]. It may indicate that longer duration of ILC for these head and neck cancer survivors may be related to the specific cancer site.
For LCD, normal controls exhibited an average duration of approximately 0.72 seconds. The head and neck cancer survivors differed significantly, reaching approximately 1.5 seconds for the duration of laryngeal closure. As stated previously, this could be due to the effects of cancer intervention, leading to difficulties with airway protection. Four head and neck cancer survivors that had a mean length of LCD over 2 seconds aspirated. Even though these survivors showed longer LCD, their delayed initiation of laryngeal closure and lack of responsiveness contributed to aspiration. Further research needs to be conducted to compare the relationship of ILC and LCD for the head and neck cancer survivors exhibited aspiration.
The stroke survivors’ LCD did not differ significantly from the healthy controls. These results are consistent with those of a previous study [18]. Power et al. [18] noted that non-aspirating stroke survivors did not differ from the normal controls. In our study, only one stroke survivor of the group aspirated. This individual exhibited a significantly lengthier and abnormal LCD (4.85 seconds).
It is important to note that both groups, stroke survivors and head and neck cancer survivors, exhibited longer LCD compared to the healthy controls. This could be a result of a compensatory mechanism in both populations in attempts to protect themselves from aspiration, but it was not always successful.
CLINICAL IMPLICATIONS
The results of this study provided evidence that clinicians should focus on specific swallowing pathophysiology for each survivor group. For stroke survivors, initiation of laryngeal closure swallow should be observed closely during instrumental evaluation and intervention. For head and neck survivors, it is important to observe the duration of laryngeal closure.
Due to the delayed initiation of laryngeal closure, clinicians need to be aware of the intervention approaches to limit this pharyngeal delay. Examples of compensatory mechanisms that can assist with a delayed pharyngeal swallow include the chin tuck and thermal gustatory stimulation [19,20]. During the chin tuck, there is a narrowing of the laryngeal area of the pharynx, which compensates for the delayed pharyngeal swallow [19]. Thermal gustatory stimulation refers to the stroking of a cold or sour item on the anterior faucial pillars of the patient before they initiate swallowing [20].
For LCD, the individuals with the longest durations were also individuals who aspirated. This may provide evidence that these survivors with a longer LCD are aspirators due to delayed initiation of laryngeal closure. Further, these individuals show more efforts to protect their airway by holding prolonged laryngeal closure duration to compensate for delayed laryngeal closure. It is important for clinicians to closely observe the relation between delayed and prolonged laryngeal closure patterns in these populations with dysphagia. It is not clear whether prolonged laryngeal closure helps to compensate for delayed initiation of laryngeal closure. The supraglottic swallow could be a useful compensatory technique for patients with prolonged LCD [21]. This strategy may assist the patient with closing the airway prior to swallow initiation so that the sensory and motor systems have already been informed. Patients should also cough following the swallow to prevent any post-swallow aspiration. Once this strategy is used in conjunction with diet modification, survivors may show evidence of safer swallowing.
LIMITATIONS
There were some limitations to this study. First, there were a small number of participants, 15 individuals in each group. Further studies should include larger sample sizes per group to better assess differences. In addition, within each group, there was variability (e.g., lesion location, location of cancer, and type of treatment). The range of heterogeneity in this study should be noted; however, this was a preliminary study looking at general group differences. Further studies should take these different components into consideration when comparing these populations.